LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



Does GLP-1 help with belly fat? GLP-1 receptor agonists like semaglutide and tirzepatide produce substantial weight loss, including significant reductions in abdominal fat and waist circumference. While these medications don't selectively target belly fat, clinical trials demonstrate meaningful decreases in visceral adipose tissue—the metabolically harmful fat surrounding internal organs—as part of overall fat loss. Studies show waist circumference reductions of 9-18 cm alongside improvements in cardiometabolic health markers. Understanding how GLP-1 medications affect abdominal fat distribution helps set realistic expectations for patients considering these therapies for weight management.
Quick Answer: GLP-1 receptor agonists produce significant reductions in abdominal fat and waist circumference as part of generalized weight loss, though they do not selectively target belly fat.
We offer compounded medications and Zepbound®. Compounded medications are prepared by licensed pharmacies and are not FDA-approved. References to Wegovy®, Ozempic®, Rybelsus®, Mounjaro®, or Saxenda®, or other GLP-1 brands, are informational only. Compounded and FDA-approved medications are not interchangeable.
Glucagon-like peptide-1 (GLP-1) receptor agonists are a class of medications originally developed for type 2 diabetes management that have demonstrated significant weight loss effects. These medications mimic the action of naturally occurring GLP-1, an incretin hormone released by the intestine in response to food intake. FDA-approved GLP-1 receptor agonists include semaglutide (Ozempic, Wegovy), liraglutide (Victoza, Saxenda), and dulaglutide (Trulicity). Tirzepatide (Mounjaro, Zepbound) is a dual GIP/GLP-1 receptor agonist that acts on both pathways.
The mechanism of action involves multiple physiological pathways that contribute to weight reduction. GLP-1 receptor agonists enhance glucose-dependent insulin secretion from pancreatic beta cells while suppressing inappropriate glucagon release, thereby improving glycemic control. More relevant to weight loss, these medications slow gastric emptying, which prolongs satiety and reduces appetite. They also act on appetite-regulating centers in the hypothalamus, decreasing hunger signals and food cravings. GLP-1 receptors are found throughout the body, including in adipose tissue, though their direct metabolic effects on fat cells in humans remain an area of active investigation.
These medications are administered via subcutaneous injection, typically weekly for semaglutide and dulaglutide, or daily for liraglutide. The dosing is gradually titrated upward over several weeks to minimize gastrointestinal side effects. According to the American Diabetes Association guidelines, GLP-1 receptor agonists are recommended as preferred agents for patients with type 2 diabetes who require weight loss. For chronic weight management, the FDA has approved specific formulations—Wegovy (semaglutide 2.4 mg), Saxenda (liraglutide 3.0 mg), and Zepbound (tirzepatide)—for adults with obesity (BMI ≥30 kg/m²) or overweight (BMI ≥27 kg/m²) with at least one weight-related comorbidity.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Clinical trials have demonstrated that GLP-1 receptor agonists produce substantial reductions in total body weight, with emerging evidence suggesting effects on visceral adipose tissue—the metabolically active fat stored around abdominal organs. The STEP (Semaglutide Treatment Effect in People with obesity) trials showed that semaglutide 2.4 mg weekly resulted in mean weight loss of 12-15% over 68 weeks compared to placebo. Importantly, body composition analyses using dual-energy X-ray absorptiometry (DEXA) and magnetic resonance imaging (MRI) have revealed that a significant proportion of this weight loss comes from fat mass rather than lean tissue.
A 2021 study published in Lancet Diabetes & Endocrinology examined body composition changes with semaglutide and found that approximately 70% of weight lost was fat mass, with notable reductions in visceral adipose tissue volume. Visceral fat, which accumulates around internal organs in the abdominal cavity, is particularly associated with metabolic complications including insulin resistance, dyslipidemia, and cardiovascular disease. Research suggests that GLP-1 medications may reduce this harmful fat depot as part of overall weight loss, though the mechanisms remain incompletely understood.
The SURMOUNT-1 trial evaluating tirzepatide for obesity demonstrated even greater weight reductions, with participants losing up to 20% of body weight at the highest dose. Waist circumference—a clinical surrogate marker for abdominal and visceral fat—decreased by approximately 14-18 cm (5.5-7.1 inches) in a dose-dependent manner over the treatment period. These findings suggest that while GLP-1 medications produce generalized fat loss throughout the body, abdominal fat deposits appear to respond as part of this overall weight reduction, likely due to the metabolically active nature of visceral adipose tissue.
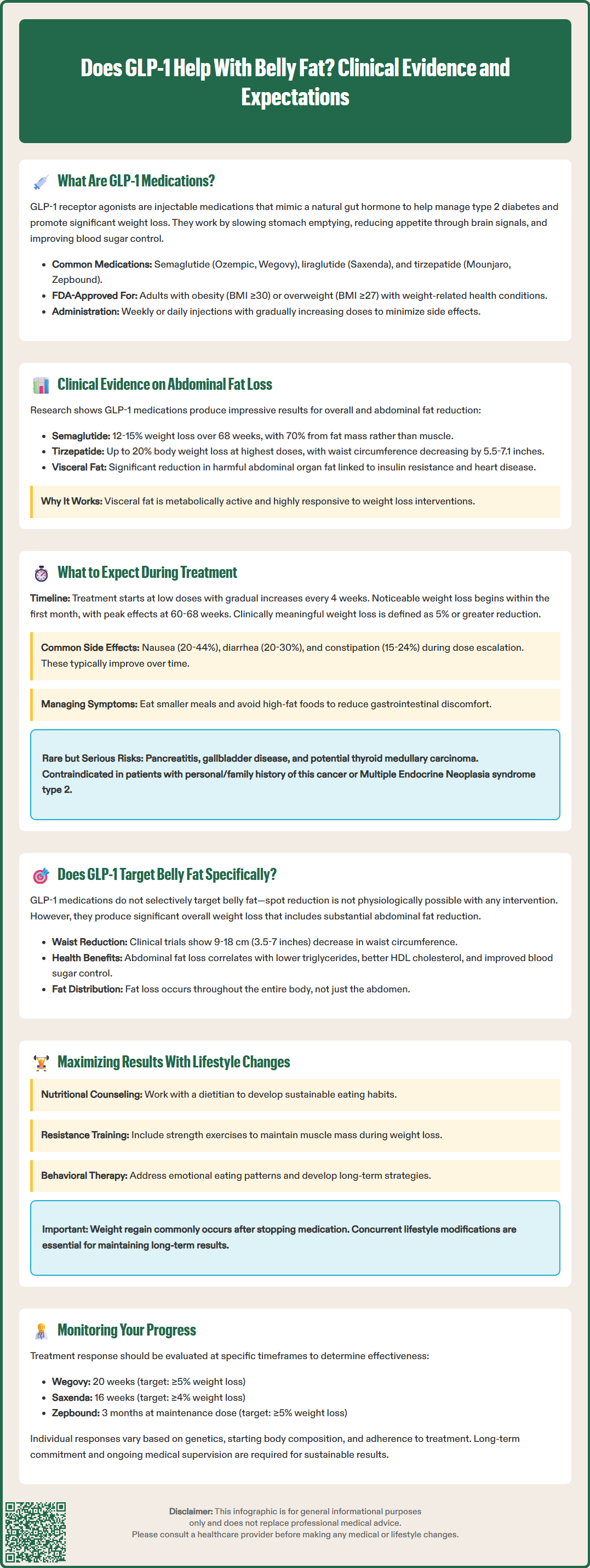
Patients initiating GLP-1 therapy for weight management should anticipate a gradual titration schedule designed to minimize adverse effects while optimizing therapeutic response. Treatment typically begins at a low dose with incremental increases every 4 weeks until reaching the maintenance dose or the maximum tolerated dose. Weight loss generally becomes noticeable within the first month, with peak effects occurring between 60-68 weeks of continuous therapy. The American College of Physicians recommends setting realistic expectations: clinically meaningful weight loss is defined as 5% or greater reduction in baseline body weight.
Common adverse effects include gastrointestinal symptoms, which affect the majority of patients to varying degrees:
Nausea (20-44% of patients) — usually most pronounced during dose escalation
Diarrhea (20-30%)
Constipation (15-24%)
Vomiting (9-24%)
Abdominal pain (6-10%)
These symptoms typically diminish over time as physiological adaptation occurs. Eating smaller, more frequent meals and avoiding high-fat foods can help manage gastrointestinal side effects. More serious but rare adverse effects include pancreatitis, gallbladder disease, and potential thyroid C-cell tumors (based on rodent studies; human relevance uncertain). The FDA label carries a boxed warning regarding thyroid medullary carcinoma risk, contraindicating use in patients with personal or family history of this condition or Multiple Endocrine Neoplasia syndrome type 2.
Patients should be monitored regularly for treatment response, tolerability, and potential complications. Healthcare providers typically assess weight, waist circumference, blood pressure, and metabolic parameters at baseline and during follow-up visits. Continuation criteria vary by medication: for Wegovy, evaluate at 20 weeks with a target of ≥5% weight loss; for Saxenda, evaluate at 16 weeks with a target of ≥4% weight loss; for Zepbound, evaluate after 3 months at maintenance dose with a target of ≥5% weight loss.
Additional safety considerations include: risk of hypoglycemia when used with insulin or sulfonylureas (dose adjustments may be needed); potential worsening of diabetic retinopathy with semaglutide in patients with pre-existing retinopathy; contraindication during pregnancy and breastfeeding; and possible need to adjust medication timing before procedures involving anesthesia due to delayed gastric emptying. Patients should seek immediate medical attention for severe persistent abdominal pain (possible pancreatitis), right upper quadrant pain with fever or jaundice (possible gallbladder disease), or signs of dehydration.
Importantly, weight regain commonly occurs after medication cessation, emphasizing the need for concurrent lifestyle modifications including dietary changes and increased physical activity to maintain long-term results.
While GLP-1 receptor agonists produce significant overall weight loss, there is no definitive evidence that they selectively target abdominal fat to the exclusion of fat in other body regions. However, clinical studies consistently demonstrate substantial reductions in waist circumference and visceral adipose tissue volume, suggesting that abdominal fat responds as part of generalized fat loss with these medications. The apparent effects on visceral fat may be explained by the metabolically active nature of this tissue and its response to overall weight reduction.
Visceral adipose tissue exhibits greater lipolytic activity compared to subcutaneous fat, though it is typically more insulin resistant. As GLP-1 therapy leads to weight loss, improved glycemic control, and potentially reduced inflammation, visceral fat deposits may decrease along with fat in other areas. The appetite suppression and caloric restriction achieved with GLP-1 treatment create an energy deficit that the body addresses by mobilizing stored fat throughout the body, including visceral depots.
From a clinical perspective, patients using GLP-1 medications can expect meaningful reductions in abdominal girth and visceral fat as part of comprehensive weight loss. The STEP 1 trial reported waist circumference reductions of approximately 9-10 cm with semaglutide 2.4 mg, while the SURMOUNT-1 trial showed reductions of 14-18 cm with tirzepatide, depending on dose. These changes correlate with improved cardiometabolic risk markers including reduced triglycerides, improved HDL cholesterol, and better glycemic control. However, it is important to emphasize that spot reduction—losing fat from one specific area while preserving it elsewhere—is not physiologically possible with any intervention, including GLP-1 therapy.
Patient counseling should include:
Realistic expectations about generalized rather than targeted fat loss
The importance of combining medication with lifestyle modifications
Recognition that individual response varies based on genetics, baseline body composition, and adherence
Understanding that sustainable results require long-term commitment
For optimal outcomes, GLP-1 therapy should be integrated into a comprehensive weight management program that includes nutritional counseling, regular physical activity (particularly resistance training to preserve lean muscle mass), behavioral therapy, and ongoing medical supervision. Patients experiencing inadequate response or intolerable side effects should be referred back to their prescribing physician for dose adjustment or consideration of alternative weight management strategies.
GLP-1 medications do not selectively target belly fat but produce generalized fat loss throughout the body, including significant reductions in abdominal and visceral fat. Clinical trials consistently show substantial waist circumference decreases as part of overall weight loss.
Clinical trials demonstrate waist circumference reductions of approximately 9-10 cm with semaglutide and 14-18 cm with tirzepatide over treatment periods of 60-72 weeks. Individual results vary based on baseline body composition, adherence, and lifestyle factors.
Visceral fat is metabolically active fat stored around abdominal organs that increases risk for insulin resistance, cardiovascular disease, and metabolic complications. GLP-1 medications reduce visceral adipose tissue volume alongside overall fat loss, improving cardiometabolic health markers.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.