LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible




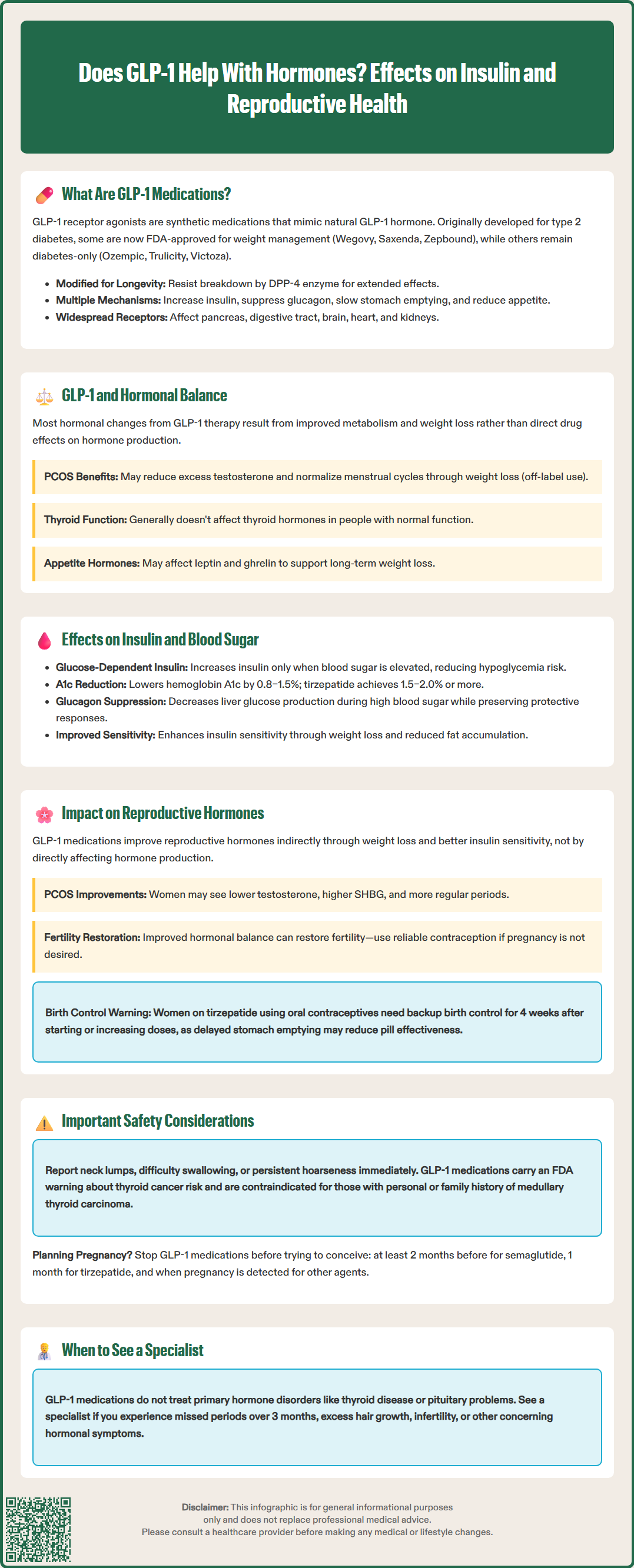
Does GLP-1 help with hormones? GLP-1 receptor agonists like semaglutide (Ozempic, Wegovy) and tirzepatide (Mounjaro, Zepbound) are FDA-approved medications primarily used for type 2 diabetes and chronic weight management. While not classified as hormonal therapies, these agents can indirectly influence hormonal balance through weight loss and improved insulin sensitivity. Evidence suggests potential benefits for reproductive hormones in conditions like polycystic ovary syndrome (PCOS), though most hormonal effects appear secondary to metabolic improvements rather than direct hormonal modulation. Understanding these complex interactions is essential for appropriate patient counseling and clinical decision-making.
Quick Answer: GLP-1 receptor agonists primarily influence hormones indirectly through weight loss and improved insulin sensitivity rather than direct hormonal modulation.
We offer compounded medications and Zepbound®. Compounded medications are prepared by licensed pharmacies and are not FDA-approved. References to Wegovy®, Ozempic®, Rybelsus®, Mounjaro®, or Saxenda®, or other GLP-1 brands, are informational only. Compounded and FDA-approved medications are not interchangeable.
Glucagon-like peptide-1 (GLP-1) receptor agonists are a class of medications originally developed for type 2 diabetes management. While some are FDA-approved for chronic weight management (Wegovy, Saxenda, Zepbound), others are approved only for diabetes (Ozempic, Trulicity, Victoza). These medications include semaglutide (Ozempic, Wegovy), dulaglutide (Trulicity), liraglutide (Victoza, Saxenda), and tirzepatide (Mounjaro, Zepbound)—with tirzepatide being a dual GIP/GLP-1 receptor agonist rather than a pure GLP-1 agonist.
GLP-1 is itself a naturally occurring incretin hormone produced by intestinal L-cells in response to food intake. The synthetic GLP-1 receptor agonists mimic this endogenous hormone but are structurally modified to resist rapid enzymatic degradation by dipeptidyl peptidase-4 (DPP-4), resulting in prolonged therapeutic activity. These medications work through multiple complementary mechanisms: they enhance glucose-dependent insulin secretion from pancreatic beta cells, suppress inappropriate glucagon release from alpha cells, slow gastric emptying to reduce postprandial glucose excursions, and act on central nervous system pathways to promote satiety and reduce appetite.
The pharmacological effects extend beyond simple glucose control. By engaging GLP-1 receptors distributed throughout various organ systems—including the pancreas, gastrointestinal tract, brain, heart, and kidneys—these agents influence multiple physiological processes. The delayed gastric emptying can also affect the absorption of some oral medications, which has clinical implications for drug interactions.
Understanding the broad mechanism of action is essential when considering whether GLP-1 medications might influence hormonal balance more generally, particularly given their increasing use in diverse patient populations including those with metabolic syndrome, polycystic ovary syndrome (PCOS), and obesity-related endocrine dysfunction.
Current evidence regarding GLP-1 receptor agonists and broader hormonal effects remains an evolving area of investigation. While these medications are not primarily classified as hormonal therapies, their metabolic effects inevitably intersect with endocrine function, particularly in patients with obesity and insulin resistance—conditions known to disrupt multiple hormonal axes.
Clinical studies have documented indirect hormonal benefits primarily mediated through weight loss and improved insulin sensitivity. In patients with obesity, significant weight reduction achieved with GLP-1 therapy has been associated with improvements in sex hormone-binding globulin (SHBG) levels, reductions in free testosterone in women with hyperandrogenism, and normalization of menstrual cycles in some individuals with polycystic ovary syndrome (PCOS). These applications represent off-label use, and the evidence is primarily from small trials and observational studies. It remains uncertain whether these effects result directly from GLP-1 receptor activation or secondarily from metabolic improvement and adipose tissue reduction.
Research into thyroid function has shown that GLP-1 agonists do not typically alter thyroid hormone levels in patients with normal thyroid function, though TSH may decrease with weight loss. The FDA-mandated boxed warning regarding medullary thyroid carcinoma stems from rodent studies showing C-cell hyperplasia and tumors at clinically relevant exposures; human relevance remains uncertain, and these medications are contraindicated in patients with personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2. Patients should be counseled to report symptoms such as neck mass, dysphagia, or persistent hoarseness for prompt evaluation.
Studies examining cortisol, growth hormone, and other pituitary hormones have generally not demonstrated clinically significant direct effects, though data are limited. Most observed hormonal changes appear to be secondary consequences of improved metabolic health rather than primary pharmacological actions. Ongoing research continues to explore potential effects on appetite-regulating hormones including leptin, ghrelin, and peptide YY, with preliminary data suggesting complex interactions that may contribute to sustained weight loss beyond simple caloric restriction.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

The most well-established hormonal effects of GLP-1 receptor agonists involve the glucose-regulatory hormone system, specifically insulin and glucagon. These medications fundamentally alter pancreatic islet cell function in a glucose-dependent manner, which provides both therapeutic efficacy and an important safety advantage over older diabetes medications.
GLP-1 agonists enhance insulin secretion from pancreatic beta cells only when blood glucose levels are elevated, a mechanism termed "glucose-dependent insulinotropic action." This physiological approach reduces the risk of hypoglycemia compared with sulfonylureas or exogenous insulin, though the risk increases when GLP-1 agents are combined with insulin or sulfonylureas, potentially requiring dose adjustments of these medications. The enhanced insulin response improves postprandial glucose control and reduces hemoglobin A1c levels by approximately 0.8–1.5% for GLP-1 receptor agonists, while the dual GIP/GLP-1 agonist tirzepatide often achieves greater reductions of 1.5–2.0% or more in clinical trials.
Simultaneously, these agents suppress glucagon secretion from pancreatic alpha cells, particularly during hyperglycemic states. Glucagon is a counter-regulatory hormone that stimulates hepatic glucose production; its inappropriate elevation contributes to fasting hyperglycemia in type 2 diabetes. By reducing excessive glucagon release, GLP-1 agonists decrease hepatic glucose output and improve overall glycemic control. Importantly, this suppression is also glucose-dependent—glucagon responses to hypoglycemia remain intact, preserving a critical protective mechanism.
Beyond direct pancreatic effects, GLP-1 therapy is associated with improved insulin sensitivity in peripheral tissues, particularly skeletal muscle and adipose tissue. This effect appears primarily mediated by weight loss and reduction in ectopic fat deposition in humans, though some preclinical evidence suggests potential direct effects on insulin signaling pathways. Patients typically experience reductions in fasting insulin levels and improved HOMA-IR (Homeostatic Model Assessment for Insulin Resistance) scores, indicating enhanced insulin sensitivity. These metabolic improvements can have cascading effects on other hormone systems disrupted by insulin resistance, including sex hormones and inflammatory mediators.
The relationship between GLP-1 receptor agonists and reproductive hormones is complex and primarily indirect, mediated through improvements in metabolic health rather than direct hormonal modulation. This distinction is clinically important when counseling patients about expected effects and appropriate monitoring.
In women with polycystic ovary syndrome (PCOS) and obesity, GLP-1 therapy has shown promise in improving reproductive hormone profiles, though this represents an off-label use with limited evidence. Clinical studies have documented reductions in total and free testosterone levels, increases in SHBG, and improvements in menstrual regularity following treatment with liraglutide or semaglutide. These changes appear to result from weight loss and improved insulin sensitivity rather than direct ovarian effects. Insulin resistance and compensatory hyperinsulinemia stimulate ovarian androgen production and suppress hepatic SHBG synthesis; by addressing these underlying metabolic abnormalities, GLP-1 agonists can indirectly normalize androgen levels. Some women experience restoration of ovulatory cycles, which has important implications for contraceptive counseling—patients should be advised that fertility may improve, and reliable contraception is essential if pregnancy is not desired.
For male patients, limited data suggest potential improvements in testosterone levels in men with obesity and hypogonadism, likely secondary to weight loss and reduced aromatase activity in adipose tissue. However, GLP-1 agonists are not indicated as primary therapy for hypogonadism, and patients with persistent symptoms should undergo appropriate endocrine evaluation.
Important safety considerations include the lack of data regarding GLP-1 use during pregnancy. These medications should be discontinued before planned conception according to drug-specific guidelines: at least 2 months before for semaglutide, at least 1 month for tirzepatide, and when pregnancy is recognized for other agents. Women taking tirzepatide who use oral contraceptives should be advised that delayed gastric emptying may reduce contraceptive efficacy; backup contraception is recommended for 4 weeks after initiation and dose escalation. There is limited data on use during breastfeeding; patients should discuss risks and benefits with their healthcare provider.
There is no established role for GLP-1 therapy in treating primary hormonal disorders such as thyroid disease, adrenal insufficiency, or pituitary dysfunction—these conditions require specific hormone replacement or disease-directed therapy. Patients experiencing concerning reproductive or endocrine symptoms (amenorrhea >3 months, virilization, infertility, or suspected endocrine disease) should be referred to endocrinology or OB-GYN specialists rather than assuming GLP-1 therapy will address underlying endocrine pathology.
GLP-1 receptor agonists may improve reproductive hormone profiles in women with PCOS through weight loss and improved insulin sensitivity, potentially reducing testosterone levels and restoring menstrual regularity. However, this represents off-label use with limited evidence, and effects are primarily indirect rather than direct hormonal modulation.
GLP-1 agonists do not typically alter thyroid hormone levels in patients with normal thyroid function, though TSH may decrease with weight loss. These medications are contraindicated in patients with personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2.
Yes, GLP-1 medications should be discontinued before planned conception: at least 2 months before for semaglutide, at least 1 month for tirzepatide, and when pregnancy is recognized for other agents. Fertility may improve with treatment, so reliable contraception is essential if pregnancy is not desired.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.