LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



Tirzepatide (Mounjaro, Zepbound) is a dual GIP/GLP-1 receptor agonist approved for type 2 diabetes and chronic weight management. While the medication has well-documented gastrointestinal side effects, patients occasionally ask whether tirzepatide causes allodynia—a condition where normally painless stimuli trigger pain. Understanding the established side effect profile of tirzepatide and the nature of allodynia helps patients and clinicians distinguish medication-related symptoms from other causes. This article examines the evidence regarding tirzepatide and allodynia, reviews common adverse effects, and provides guidance on when neurological symptoms require medical evaluation.
Quick Answer: There is currently no established link between tirzepatide and allodynia in FDA prescribing information or published clinical trial data.
Tirzepatide is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist approved by the FDA for the treatment of type 2 diabetes mellitus (Mounjaro) and chronic weight management (Zepbound). For weight management, it's indicated for adults with a BMI ≥30 kg/m² or ≥27 kg/m² with at least one weight-related comorbidity.
The medication works through a dual mechanism of action by simultaneously activating both GIP and GLP-1 receptors. This dual agonism enhances insulin secretion in a glucose-dependent manner, meaning insulin is released only when blood glucose levels are elevated, thereby reducing the risk of hypoglycemia. Additionally, tirzepatide suppresses glucagon secretion, slows gastric emptying, and promotes satiety through central nervous system pathways that regulate appetite.
Clinical trials have demonstrated that tirzepatide produces substantial reductions in hemoglobin A1c levels (up to 2.5% in some studies) and significant weight loss (approximately 15-21% of body weight in obesity trials at the highest doses, with somewhat lower percentages in type 2 diabetes trials). The medication is administered once weekly via subcutaneous injection, with doses ranging from 2.5 mg to 15 mg. The starting dose is typically 2.5 mg, with gradual titration every four weeks to minimize gastrointestinal side effects and improve tolerability.
Tirzepatide is not indicated for type 1 diabetes and should be avoided during pregnancy. The delayed gastric emptying effect may reduce the absorption of oral medications, including oral contraceptives. Women using oral contraceptives should use a backup or non-oral method for 4 weeks after initiation and after each dose increase.
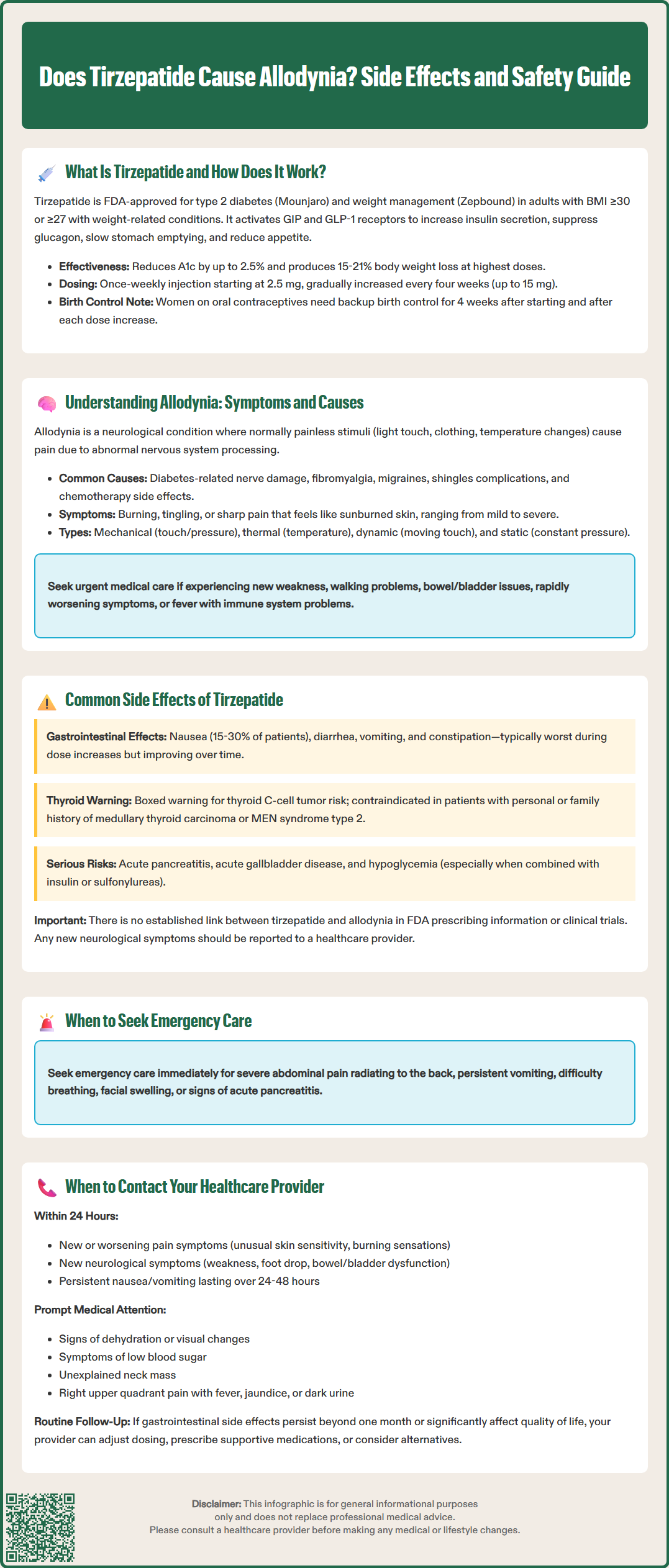
Allodynia is a neurological condition characterized by pain resulting from stimuli that normally would not provoke pain. Patients with allodynia experience discomfort from everyday sensations such as light touch, gentle pressure, or temperature changes that healthy individuals tolerate without issue. This phenomenon represents a form of neuropathic pain where the nervous system processes non-painful stimuli as painful signals.
There are several types of allodynia, classified by the triggering stimulus. Mechanical allodynia occurs with physical touch or pressure, such as clothing against skin or light brushing. Thermal allodynia involves pain from temperature changes that are normally comfortable. Dynamic allodynia results from moving stimuli across the skin, while static allodynia occurs with constant, gentle pressure. Patients may experience one or multiple types simultaneously.
The underlying causes of allodynia are diverse and include peripheral neuropathy (commonly from diabetes), fibromyalgia, complex regional pain syndrome, migraine headaches, and postherpetic neuralgia following shingles. Certain medications, particularly chemotherapy agents, can also induce allodynia as a side effect. The pathophysiology involves sensitization of peripheral nociceptors and altered central nervous system processing of sensory information.
Symptoms typically include burning, tingling, or sharp pain in response to normally innocuous stimuli. The affected areas may be localized or widespread, and the intensity can range from mild discomfort to severe, debilitating pain. Patients often describe the sensation as feeling sunburned or having extremely sensitive skin. The condition significantly impacts quality of life, affecting sleep, daily activities, and emotional well-being. Diagnosis is primarily clinical, with quantitative sensory testing used selectively in specialized settings.
Red flags requiring urgent evaluation include new focal weakness, gait disturbance, bowel or bladder dysfunction, rapidly progressive symptoms, or fever in immunocompromised patients. Initial workup may include A1c/glucose, vitamin B12, thyroid function, and comprehensive metabolic panel.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

According to FDA prescribing information, the most frequently reported adverse effects of tirzepatide are gastrointestinal in nature. Nausea is the most common side effect, affecting approximately 15-30% of patients depending on the dose, followed by diarrhea (13-16%), vomiting (6-12%), and constipation (6-7%). These symptoms are typically most pronounced during dose escalation and often diminish over time as the body adapts to the medication.
Other common side effects include decreased appetite (which contributes to weight loss), abdominal pain, dyspepsia, and gastroesophageal reflux. Injection site reactions such as redness, itching, or mild discomfort occur in approximately 2-4% of patients but are generally mild and self-limiting. Some patients report fatigue, dizziness, or headache, particularly during the initial weeks of treatment.
More serious but less common adverse effects require clinical vigilance. Tirzepatide carries a boxed warning regarding the risk of thyroid C-cell tumors, based on animal studies, though the relevance to humans remains uncertain. The medication is contraindicated in patients with a personal or family history of medullary thyroid carcinoma or multiple endocrine neoplasia syndrome type 2. Acute pancreatitis has been reported in clinical trials and post-marketing surveillance, with patients experiencing severe abdominal pain requiring immediate medical evaluation.
Tirzepatide may increase the risk of acute gallbladder disease, including cholelithiasis and cholecystitis. It is not recommended in patients with severe gastrointestinal disease, including severe gastroparesis. Zepbound (tirzepatide for weight management) carries a warning about suicidal thoughts and behaviors.
Hypoglycemia risk increases when tirzepatide is used in combination with insulin or sulfonylureas, necessitating dose adjustments of these concomitant medications. Acute kidney injury has been reported, typically in the context of severe dehydration from gastrointestinal side effects. Diabetic retinopathy complications may occur in patients with pre-existing retinopathy, particularly with rapid glycemic improvement (a phenomenon noted with any treatment causing rapid glucose lowering, not specific to tirzepatide).
There is currently no established link between tirzepatide and allodynia in the FDA-approved prescribing information or published clinical trial data. While peripheral neuropathy can occur in diabetes patients, this is typically related to the underlying disease rather than GLP-1 or GIP receptor agonist therapy. Patients experiencing new neurological symptoms should report them to their healthcare provider and consider reporting to FDA MedWatch.
Patients taking tirzepatide should be educated about warning signs that require prompt medical attention. Seek immediate emergency care if you experience severe abdominal pain that radiates to the back, persistent vomiting preventing fluid intake, signs of allergic reaction (difficulty breathing, facial swelling, severe rash), or symptoms of acute pancreatitis. These represent potentially serious complications requiring urgent evaluation.
Contact your healthcare provider within 24 hours if you develop new or worsening pain symptoms, including unusual skin sensitivity, burning sensations, or pain from normally non-painful touch. While there is no official link between tirzepatide and allodynia, any new neurological symptoms warrant clinical assessment to determine the underlying cause. Urgent neurological evaluation is needed for new focal weakness, foot drop, bowel or bladder dysfunction, or rapidly progressive symptoms.
Other situations requiring prompt communication with your provider include persistent nausea or vomiting lasting more than 24-48 hours, signs of dehydration (decreased urination, dizziness, dry mouth), visual changes, symptoms of hypoglycemia (shakiness, confusion, rapid heartbeat), or unexplained neck mass or hoarseness. Changes in urination patterns, particularly decreased urine output, may indicate kidney problems and require laboratory evaluation. Right upper quadrant pain, fever, jaundice, or dark urine could indicate gallbladder problems and require immediate attention.
For routine concerns, schedule an appointment if gastrointestinal side effects persist beyond the first month of treatment or significantly impact your quality of life. Your provider can adjust the titration schedule, provide supportive medications, or consider alternative therapies if side effects are intolerable. Regular follow-up appointments should include monitoring of hemoglobin A1c, kidney function, and assessment for diabetic complications including neuropathy. Patients with pre-existing diabetic retinopathy should maintain regular ophthalmology follow-up.
Women using oral contraceptives should discuss the potential for reduced effectiveness with their provider and consider using a backup or non-oral method for 4 weeks after tirzepatide initiation and after each dose increase. If pregnancy occurs or is planned, inform your provider immediately, as tirzepatide should be discontinued for weight management upon pregnancy recognition.
No, allodynia is not listed as an established side effect in FDA prescribing information or clinical trial data for tirzepatide. However, patients experiencing new neurological symptoms should report them to their healthcare provider for proper evaluation.
The most common side effects are gastrointestinal, including nausea (15-30%), diarrhea (13-16%), vomiting (6-12%), and constipation (6-7%). These symptoms typically occur during dose escalation and often improve over time.
Contact your healthcare provider within 24 hours if you develop new or unusual skin sensitivity, burning sensations, or pain from normally non-painful touch. Seek immediate care for severe symptoms, new weakness, or rapidly progressive neurological changes.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.