





LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



Does tirzepatide cause acid reflux? This question concerns many patients considering or currently taking this dual GIP/GLP-1 receptor agonist for type 2 diabetes or weight management. Tirzepatide (Mounjaro, Zepbound) works by slowing gastric emptying, which can lead to gastrointestinal side effects including reflux symptoms. According to FDA prescribing information, gastroesophageal reflux disease appears among common adverse reactions for Zepbound, while dyspepsia is noted for Mounjaro. Understanding the connection between tirzepatide and acid reflux helps patients and clinicians manage symptoms effectively while maintaining treatment benefits.
Quick Answer: Tirzepatide can cause acid reflux symptoms, with gastroesophageal reflux disease listed as a common adverse reaction in FDA prescribing information for Zepbound.
We offer compounded medications and Zepbound®. Compounded medications are prepared by licensed pharmacies and are not FDA-approved. References to Wegovy®, Ozempic®, Rybelsus®, Mounjaro®, or Saxenda®, or other GLP-1 brands, are informational only. Compounded and FDA-approved medications are not interchangeable.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Tirzepatide is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist approved by the FDA for type 2 diabetes management (Mounjaro) and chronic weight management (Zepbound). This medication works by enhancing insulin secretion, suppressing glucagon release, and slowing gastric emptying—mechanisms that contribute to improved glycemic control and weight loss.[1]
The pharmacological action of tirzepatide directly affects the gastrointestinal system. By delaying gastric emptying, the medication prolongs the time food remains in the stomach, which helps promote satiety and reduce caloric intake. However, this same mechanism can lead to various gastrointestinal side effects that are among the most commonly reported adverse reactions.
Common gastrointestinal side effects of tirzepatide include:
Nausea (12–24% of patients, varying by indication and dose)
Diarrhea (12–18% of patients)
Vomiting (5–10% of patients)
Constipation (5–11% of patients)
Abdominal pain or discomfort
Decreased appetite
Dyspepsia (indigestion)
These effects are typically most pronounced during the initial weeks of treatment and during dose escalation periods. The FDA prescribing information recommends gradual dose titration to minimize gastrointestinal tolerability issues.[1] Most patients experience improvement in these symptoms over time as their bodies adjust to the medication, though individual responses vary considerably. Understanding these gastrointestinal effects is essential for patients and clinicians to distinguish expected medication responses from symptoms requiring further evaluation.
| Side Effect | Frequency | Severity | Management |
|---|---|---|---|
| Nausea | 12–24% of patients | Mild to moderate; most pronounced during dose escalation | Gradual dose titration; eat smaller meals; consult provider if persistent |
| Diarrhea | 12–18% of patients | Mild to moderate | Stay hydrated; contact provider if severe or causing dehydration |
| Acid reflux / GERD | Listed as common adverse reaction in Zepbound prescribing information | Mild to moderate; may worsen with pre-existing GERD | PPIs (omeprazole, esomeprazole), antacids, H2 blockers; avoid eating 2–3 hrs before bed |
| Vomiting | 5–10% of patients | Moderate; seek care if blood present or nutrition is compromised | Slow dose titration; small frequent meals; seek emergency care if vomiting blood |
| Constipation | 5–11% of patients | Mild to moderate | Increase fluid and fiber intake; discuss laxative use with provider if needed |
| Dyspepsia (indigestion) | Listed as common adverse reaction in Mounjaro prescribing information | Mild; linked to delayed gastric emptying | Avoid trigger foods (caffeine, alcohol, spicy/fatty foods); OTC antacids for relief |
| Abdominal pain | Reported; exact frequency varies | Severe upper or back pain may indicate pancreatitis — seek emergency care | Contact provider promptly; call 911 for severe pain radiating to the back |
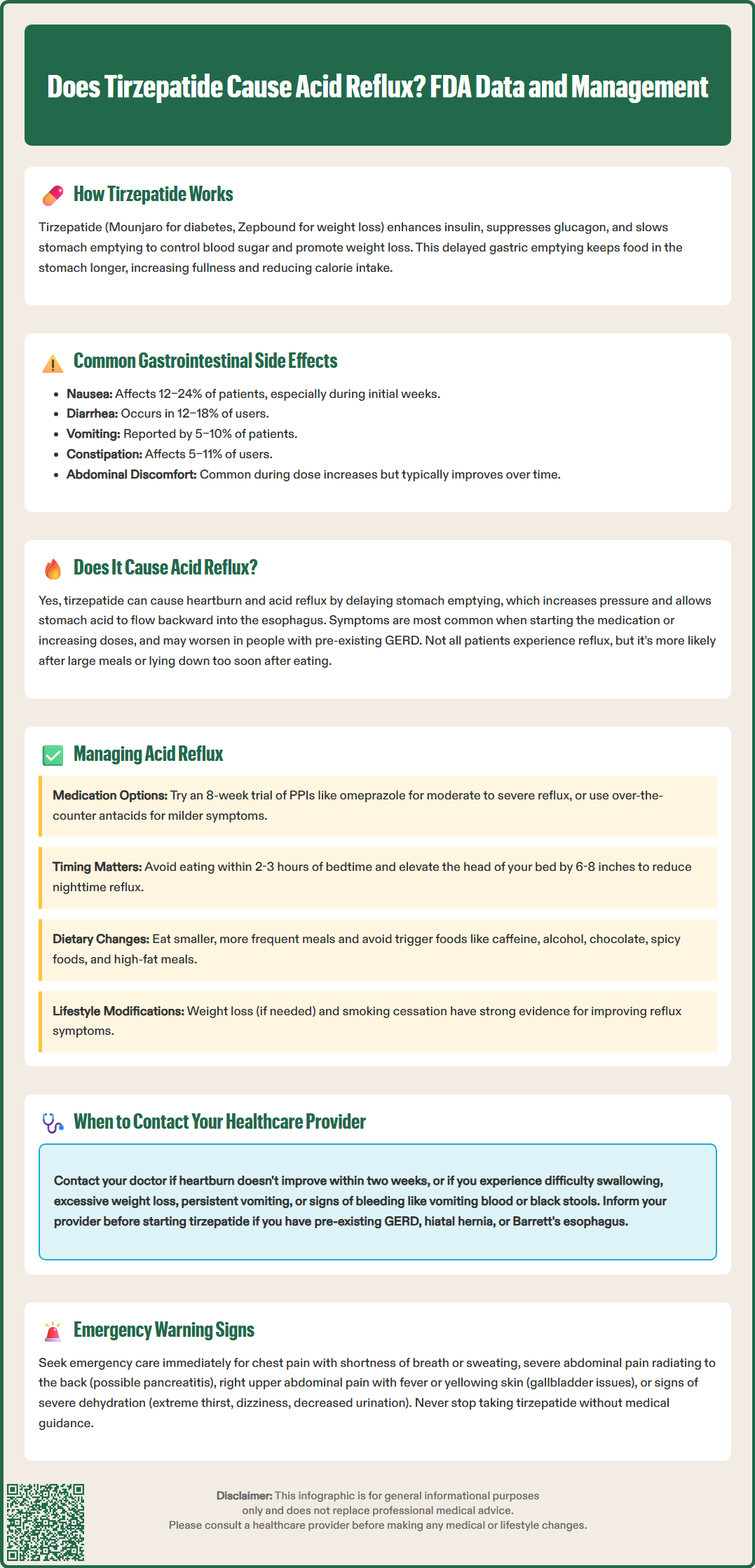
Heartburn (a burning sensation in the chest) and acid regurgitation are common symptoms of acid reflux, which can be part of gastroesophageal reflux disease (GERD) when chronic. According to the FDA-approved prescribing information, gastroesophageal reflux disease is listed among the common adverse reactions for Zepbound (tirzepatide for weight management), while dyspepsia (indigestion) is listed for Mounjaro (tirzepatide for type 2 diabetes).
There is a plausible mechanistic connection between tirzepatide use and reflux symptoms. The delayed gastric emptying caused by tirzepatide means food and gastric contents remain in the stomach for extended periods. This prolonged retention can increase intragastric pressure, potentially promoting the backward flow of stomach acid into the esophagus.[1] Additionally, the medication might theoretically influence lower esophageal sphincter function, though this specific effect has not been extensively studied.
Clinical observations suggest:
Some patients report heartburn or acid regurgitation symptoms after starting tirzepatide
Individuals with pre-existing reflux symptoms may experience exacerbation
Symptoms appear more common during initial treatment phases and dose escalation
Symptoms may correlate with larger meal sizes or lying down shortly after eating
The exact frequency of reflux symptoms varies by indication, dose, and individual patient factors. While some patients may not experience any reflux symptoms, others may find them bothersome enough to discuss with their healthcare provider. For patients with pre-existing GERD, discussing this condition before starting tirzepatide is important for appropriate monitoring and management.
For patients experiencing acid reflux symptoms while taking tirzepatide, several evidence-based management strategies can provide relief without necessarily requiring medication discontinuation. These approaches include both pharmacological interventions and lifestyle modifications appropriate for the US healthcare context.
Pharmacological management options:
According to the American College of Gastroenterology (ACG) guidelines, an 8-week trial of once-daily proton pump inhibitors (PPIs) such as omeprazole or esomeprazole is recommended as first-line therapy for typical reflux symptoms without alarm features. PPIs offer potent acid suppression for moderate to severe symptoms. For milder or occasional symptoms, over-the-counter antacids (calcium carbonate, magnesium hydroxide) can provide rapid but temporary relief. Histamine-2 receptor antagonists (H2 blockers) such as famotidine represent an intermediate option.
Long-term PPI use should be discussed with a healthcare provider, as the lowest effective dose should be used when needed for symptom control. Potential considerations with extended use include nutrient malabsorption and slightly increased infection susceptibility, though benefits often outweigh risks for those with persistent symptoms.
Lifestyle and dietary modifications:
Weight loss (if appropriate) has the strongest evidence for improving reflux symptoms[2]
Avoid eating within 2-3 hours of bedtime to reduce nighttime reflux
Elevate the head of the bed by 6–8 inches using blocks or a wedge pillow
Eat smaller, more frequent meals rather than large portions that increase gastric pressure
Identify and avoid trigger foods such as caffeine, alcohol, chocolate, spicy foods, citrus, and high-fat meals
Stop smoking, as tobacco use can worsen reflux symptoms
If gastrointestinal symptoms are severe, your healthcare provider may consider slowing the tirzepatide dose titration schedule or adjusting the maintenance dose according to FDA prescribing information.[1] Persistent symptoms despite optimal therapy warrant reassessment and possible referral to a gastroenterologist.
While mild acid reflux symptoms may be manageable with appropriate treatment, certain warning signs require prompt medical evaluation. Patients taking tirzepatide should be educated about symptoms that may indicate more serious complications or conditions requiring professional assessment.
Contact your healthcare provider if you experience:
Severe or persistent heartburn that does not respond to appropriate treatment within two weeks
Difficulty swallowing (dysphagia) or painful swallowing (odynophagia)
Weight loss that seems excessive or occurs more rapidly than expected with treatment
Persistent nausea or vomiting that prevents adequate nutrition or hydration
Vomiting blood or material that looks like coffee grounds
Black, tarry stools suggesting gastrointestinal bleeding
Severe abdominal pain, particularly if localized to the upper abdomen
Right upper abdominal pain, fever, or yellowing of skin/eyes, which may suggest gallbladder disease
Signs of dehydration such as extreme thirst, dizziness, or decreased urination after significant vomiting or diarrhea
Seek emergency care immediately (call 911) if you experience:
Chest pain, especially if accompanied by shortness of breath, sweating, or radiation to the arm or jaw
Severe, persistent abdominal pain radiating to the back, which may indicate pancreatitis
Pancreatitis is a known risk with GLP-1 receptor agonists including tirzepatide, as noted in the FDA prescribing information.[1] Additionally, patients with pre-existing GERD, hiatal hernia, or Barrett's esophagus should inform their healthcare provider before starting tirzepatide, as closer monitoring may be appropriate. Your provider can assess whether symptoms represent expected medication effects, require additional investigation such as upper endoscopy, or necessitate treatment modification. Never discontinue tirzepatide without medical guidance, as abrupt cessation may affect glycemic control in patients with diabetes.
Gastroesophageal reflux disease is listed as a common adverse reaction in FDA prescribing information for Zepbound (tirzepatide for weight management), while dyspepsia appears for Mounjaro (tirzepatide for diabetes). Exact frequency varies by dose and individual patient factors, with symptoms typically more pronounced during initial treatment and dose escalation.
Yes, over-the-counter antacids can provide rapid relief for mild symptoms, while proton pump inhibitors like omeprazole are recommended as first-line therapy for moderate to severe reflux symptoms according to American College of Gastroenterology guidelines. Discuss long-term PPI use with your healthcare provider to determine the lowest effective dose.
Contact your healthcare provider if you experience severe or persistent heartburn not responding to treatment within two weeks, difficulty swallowing, vomiting blood, black tarry stools, or severe abdominal pain. Seek emergency care immediately for chest pain or severe persistent abdominal pain radiating to the back, which may indicate pancreatitis.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.



