LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



Glucagon-like peptide-1 (GLP-1) receptor agonists, medications FDA-approved for type 2 diabetes and chronic weight management, are generating scientific interest for potential effects on substance use disorder. These drugs work throughout the body, including brain regions involved in reward processing and addiction neurobiology. Emerging preclinical research and patient reports suggest GLP-1 medications may influence cravings and consumption patterns for alcohol, tobacco, and other substances. However, there is currently no FDA indication for treating substance use disorders with these agents, and evidence remains preliminary. Understanding this evolving research area is important for clinicians managing patients with both metabolic conditions and substance use history.
Quick Answer: GLP-1 receptor agonists may influence substance use behaviors through effects on brain reward circuits, but they currently have no FDA approval for treating substance use disorders.
We offer compounded medications and Zepbound®. Compounded medications are prepared by licensed pharmacies and are not FDA-approved. References to Wegovy®, Ozempic®, Rybelsus®, Mounjaro®, or Saxenda®, or other GLP-1 brands, are informational only. Compounded and FDA-approved medications are not interchangeable.
Glucagon-like peptide-1 (GLP-1) receptor agonists are a class of medications originally developed for type 2 diabetes management. While most are approved only for diabetes, specific agents in this class have received FDA approval for chronic weight management. These medications include semaglutide (Ozempic for diabetes; Wegovy for weight management), liraglutide (Victoza for diabetes; Saxenda for weight management), dulaglutide (Trulicity for diabetes), and tirzepatide (Mounjaro for diabetes; Zepbound for weight management), with tirzepatide functioning as a dual GIP/GLP-1 receptor agonist.
GLP-1 receptor agonists work by mimicking the action of endogenous GLP-1, an incretin hormone released from intestinal L-cells in response to food intake. These medications bind to GLP-1 receptors located throughout the body, including the pancreas, gastrointestinal tract, and importantly, the central nervous system. In the pancreas, they enhance glucose-dependent insulin secretion and suppress glucagon release, improving blood sugar control with a low risk of hypoglycemia when used alone (though risk increases when combined with insulin or sulfonylureas). In the gastrointestinal system, they slow gastric emptying and reduce appetite, contributing to weight loss.
The presence of GLP-1 receptors in brain regions involved in reward processing, including the mesolimbic dopamine system, has generated scientific interest in potential effects beyond metabolic regulation. These receptors are found in areas such as the ventral tegmental area, nucleus accumbens, and prefrontal cortex—regions critically involved in addiction neurobiology. This neuroanatomical distribution has prompted researchers to investigate whether GLP-1 receptor agonists might influence addictive behaviors, leading to emerging research on their potential role in substance use disorders.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

The potential connection between GLP-1 receptor agonists and substance use disorder emerged from preclinical animal studies and subsequent anecdotal patient reports. There is no official FDA indication for GLP-1 medications in treating substance use disorders, and the relationship remains an area of active investigation rather than established clinical practice. However, accumulating evidence suggests these medications may influence reward-seeking behaviors and consumption patterns for various substances.
The proposed mechanism involves GLP-1 receptor activation in brain reward circuits that overlap with pathways implicated in addiction. Preclinical studies in rodents have demonstrated that GLP-1 receptor agonists can reduce self-administration of alcohol, nicotine, cocaine, and opioids. These effects appear to be mediated through modulation of dopamine signaling in the mesolimbic reward system in animal models, potentially dampening the reinforcing properties of addictive substances. The medications may also affect stress-related relapse mechanisms and compulsive consumption patterns in preclinical research.
Patient reports and observational data have described reduced cravings and decreased consumption of alcohol, tobacco, and other substances among individuals prescribed GLP-1 receptor agonists for diabetes or weight management. Some patients have reported spontaneous reduction in alcohol intake or loss of interest in drinking without specifically intending to change these behaviors. While these anecdotal accounts are compelling, they do not establish causation and may reflect multiple confounding factors including weight loss, improved metabolic health, or lifestyle changes.
It is important to emphasize that current evidence does not support prescribing GLP-1 medications specifically for substance use disorders outside of research settings. The observations remain preliminary, and rigorous clinical trials are needed to establish efficacy, optimal dosing, and safety profiles for this potential indication.
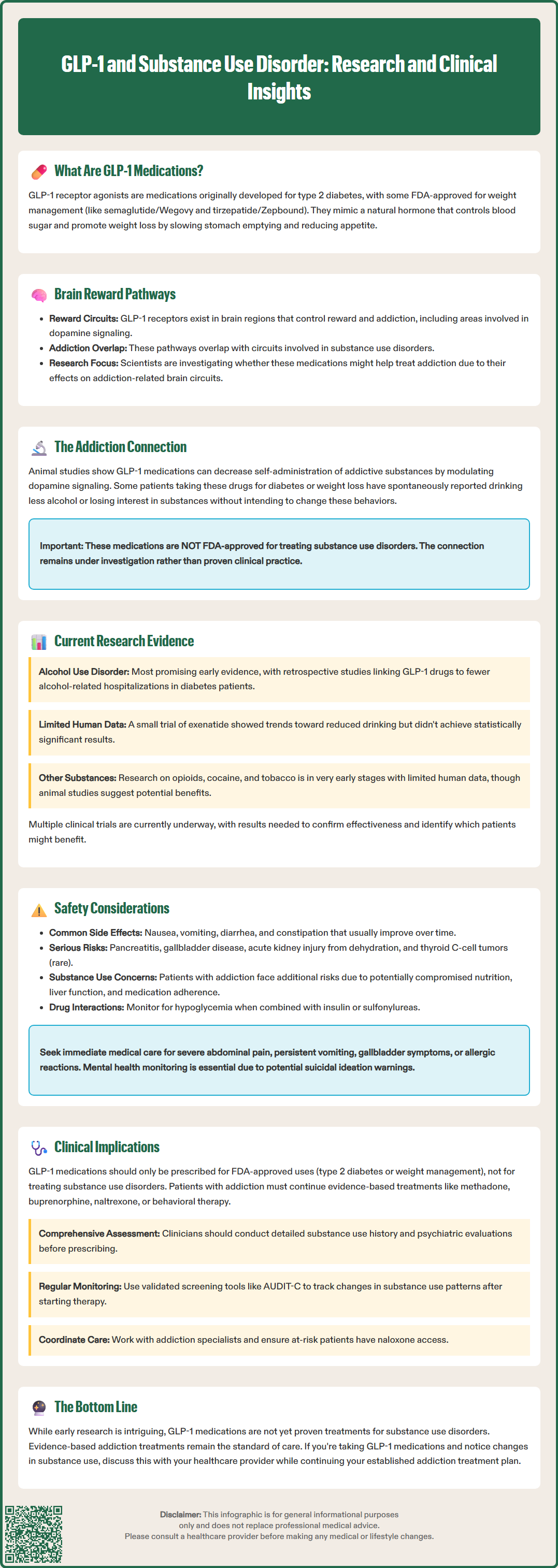
Research investigating GLP-1 receptor agonists for substance use disorders is rapidly expanding, with studies examining multiple substance classes and patient populations. Several clinical trials are currently underway or recently completed, though published results remain limited. The strongest preliminary evidence exists for alcohol use disorder, where both retrospective analyses and small prospective studies have shown promising signals.
Retrospective cohort studies using healthcare databases have found associations between GLP-1 receptor agonist use and reduced alcohol-related outcomes. For example, patients with type 2 diabetes prescribed GLP-1 receptor agonists have shown lower rates of alcohol-related hospitalizations and emergency department visits compared to those receiving other diabetes medications in some analyses. However, these retrospective studies cannot establish causation and may be influenced by unmeasured confounders or selection bias.
Small pilot studies have examined GLP-1 receptor agonists in individuals with alcohol use disorder. One randomized controlled trial of exenatide in patients with obesity and alcohol use disorder found trends toward reduced drinking, though results did not reach statistical significance in the primary outcome. Several ongoing clinical trials are evaluating semaglutide specifically for alcohol use disorder, with results pending.
Research on other substances is more preliminary. Studies are investigating GLP-1 receptor agonists for opioid use disorder, cocaine use disorder, and tobacco use disorder. Preclinical evidence supports potential efficacy across these substance classes, but human data remain sparse. Multiple investigator-initiated trials are in progress. Results from these rigorous clinical trials will be essential to determine whether GLP-1 medications have a legitimate role in addiction treatment and to identify which patient populations might benefit most.
GLP-1 receptor agonists have well-characterized safety profiles based on extensive use in diabetes and obesity management, but specific considerations apply when considering their use in patients with substance use disorders. The most common adverse effects are gastrointestinal, including nausea, vomiting, diarrhea, and constipation. These symptoms typically occur early in treatment and often diminish with continued use, though they can be dose-limiting in some patients. Gradual dose titration, as recommended in FDA labeling, helps minimize these effects.
More serious but less common adverse effects include pancreatitis, gallbladder disease (cholecystitis and cholelithiasis), and acute kidney injury, particularly in the setting of severe dehydration from gastrointestinal symptoms. The FDA labeling includes boxed warnings about thyroid C-cell tumors based on rodent studies, contraindicating use in patients with personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2. Patients with a history of pancreatitis may require alternative therapies or careful monitoring.
Semaglutide carries warnings about diabetic retinopathy complications, particularly in patients with pre-existing retinopathy who experience rapid improvement in blood glucose. Tirzepatide can delay gastric emptying, potentially reducing the effectiveness of oral contraceptives; backup contraception is recommended after initiation and dose escalations. GLP-1 receptor agonists are not recommended during pregnancy, and patients should discontinue treatment if pregnancy occurs. Weight-management formulations carry warnings about suicidal ideation and behavior, though the FDA has stated that current evidence is insufficient to establish a causal relationship.
In the context of substance use disorders, additional safety considerations emerge. Patients with active substance use may have compromised nutritional status, liver function, or medication adherence, potentially increasing risks. The interaction between GLP-1 medications and substances of abuse has not been systematically studied. Alcohol consumption may exacerbate gastrointestinal side effects or increase dehydration risk. Patients should be advised to maintain adequate hydration and nutrition.
Clinicians should monitor for hypoglycemia in patients taking GLP-1 receptor agonists with insulin or sulfonylureas. Regular assessment of renal function, particularly in patients with baseline kidney disease or those taking nephrotoxic substances, is prudent. Mental health monitoring is important. Patients should seek immediate medical attention for severe or persistent abdominal pain (possible pancreatitis), persistent vomiting, signs of gallbladder disease, or allergic reactions.
For clinicians managing patients with both metabolic conditions and substance use history, the emerging data on GLP-1 receptor agonists present both opportunities and uncertainties. Currently, these medications should be prescribed based on their FDA-approved indications—type 2 diabetes or chronic weight management—rather than for substance use disorder treatment. However, awareness of potential effects on substance use behaviors can inform clinical decision-making and patient counseling.
When prescribing GLP-1 receptor agonists to patients with current or past substance use disorders, comprehensive assessment is essential. This includes detailed substance use history, current use patterns, treatment engagement, and psychiatric comorbidities. Patients should be informed that while some individuals report reduced cravings or substance use, this is not an established therapeutic effect and should not replace evidence-based addiction treatment. Continued engagement with addiction specialists, behavioral interventions, and FDA-approved medications for substance use disorders remains the standard of care. These include methadone, buprenorphine, and extended-release naltrexone for opioid use disorder; naltrexone and acamprosate for alcohol use disorder; and varenicline, nicotine replacement therapy, and bupropion for tobacco use disorder.
Clinicians should monitor patients for changes in substance use patterns after initiating GLP-1 therapy. The U.S. Preventive Services Task Force recommends screening all adults for unhealthy alcohol use and providing brief counseling when indicated. Regular screening using validated tools such as the AUDIT-C for alcohol can help track changes. Coordination with addiction treatment providers facilitates comprehensive care and ensures that metabolic and addiction treatments are complementary rather than conflicting.
Patients should be counseled about realistic expectations and the importance of not discontinuing established addiction treatments. If patients report reduced cravings or substance use, this should be documented and monitored, but not interpreted as definitive treatment success without ongoing assessment. Conversely, if substance use worsens or new concerning patterns emerge, prompt referral to addiction specialists is warranted. Resources such as the SAMHSA National Helpline (1-800-662-HELP) can provide treatment referrals, and patients at risk for opioid overdose should be prescribed naloxone. As clinical trial data emerge, practice guidelines may evolve, but current management should prioritize evidence-based approaches while remaining attentive to this developing area of research.
No, GLP-1 receptor agonists currently have no FDA approval for treating substance use disorders. They are approved only for type 2 diabetes management and chronic weight management, and should be prescribed based on these indications while research continues.
GLP-1 medications activate receptors in brain reward circuits that overlap with addiction pathways. Preclinical studies suggest they may reduce substance cravings and consumption by modulating dopamine signaling, though human evidence remains preliminary and requires further clinical trials.
No, patients should continue evidence-based addiction treatments including FDA-approved medications and behavioral interventions. GLP-1 drugs are not a substitute for established substance use disorder treatments, and any changes in substance use patterns should be monitored by healthcare providers.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.