LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



Metformin and thyroid medication are commonly prescribed together for patients managing both type 2 diabetes and thyroid disorders. Metformin, a first-line diabetes medication, and levothyroxine, the standard thyroid hormone replacement, can generally be taken safely under medical supervision. While no absolute contraindication exists, emerging evidence suggests metformin may modestly influence thyroid-stimulating hormone (TSH) levels in some patients. Understanding proper timing, monitoring requirements, and potential interactions ensures optimal therapeutic outcomes. This guide provides evidence-based information on safely combining metformin and thyroid medication, helping patients and healthcare providers navigate concurrent therapy effectively.
Quick Answer: Metformin and thyroid medications can generally be taken together safely under appropriate medical supervision, though metformin may modestly influence TSH levels requiring monitoring.
Yes, metformin and thyroid medications can generally be taken together safely under appropriate medical supervision. Metformin, a first-line oral medication for type 2 diabetes, and thyroid hormone replacement therapy (most commonly levothyroxine) are frequently prescribed concurrently, particularly given the overlap between thyroid disorders and diabetes. Observational studies suggest that thyroid dysfunction occurs in patients with type 2 diabetes, though prevalence varies across different populations.
There is no absolute contraindication to combining these medications according to FDA-approved prescribing information for metformin, which does not list thyroid medications as contraindicated or requiring dose adjustment. However, healthcare providers should be aware that metformin may influence thyroid-stimulating hormone (TSH) levels in some patients, which can affect thyroid management. Additionally, changes in thyroid hormone dosing can impact glycemic control and may necessitate adjustments to diabetes medications.
The safety of this combination has been evaluated primarily in observational studies and meta-analyses. Research suggests that patients taking both medications can achieve effective glycemic control and thyroid hormone balance when appropriately monitored. The key to successful concurrent therapy lies in individualized dosing, regular laboratory monitoring, and clear communication between patients and their healthcare team.
Patients should always inform all prescribing physicians about their complete medication regimen, including over-the-counter supplements, to ensure comprehensive medication management and avoid potential complications.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Emerging evidence suggests that metformin may influence thyroid function parameters, particularly TSH levels, though the clinical significance remains under investigation. Several studies have documented modest reductions in TSH concentrations among patients taking metformin, with decreases ranging from 0.4 to 1.5 mIU/L, most consistently observed in patients with hypothyroidism or those taking levothyroxine. The mechanism underlying this effect is not fully established, and several theoretical explanations have been proposed.
One hypothesized mechanism involves metformin's effect on the hypothalamic-pituitary-thyroid axis. Researchers theorize that metformin may enhance thyroid hormone sensitivity at the cellular level or influence TSH secretion through effects on AMP-activated protein kinase (AMPK) signaling pathways. Additionally, metformin's impact on body weight and insulin resistance—both factors that can influence thyroid function—may indirectly contribute to TSH changes.
For patients with hypothyroidism taking levothyroxine, metformin initiation may lead to a decrease in TSH levels, potentially indicating improved thyroid hormone action or altered thyroid hormone requirements. Conversely, some patients may experience changes that necessitate levothyroxine dose adjustments. Meta-analyses examining this relationship have found that metformin use was associated with small but statistically significant TSH reductions, though free T4 and T3 levels typically remained stable.
It is important to note that metformin does not cause thyroid disease and there is no established causal link between metformin and thyroid dysfunction. The observed TSH changes appear to be modulatory rather than pathological. Patients with pre-existing thyroid conditions should not avoid metformin based on these findings, but rather ensure appropriate monitoring is in place to detect any clinically meaningful changes requiring intervention.
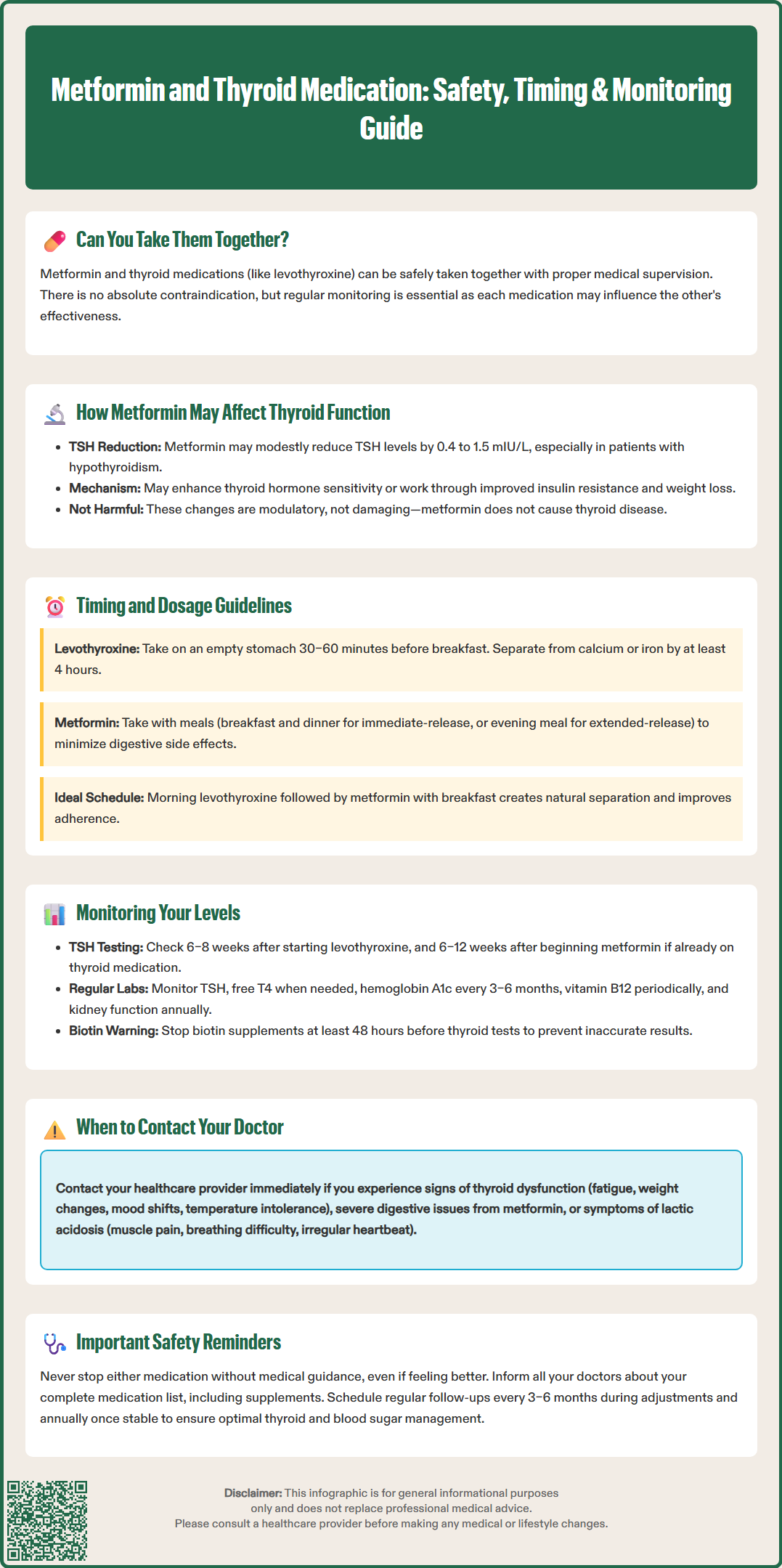
Optimal timing and dosing strategies can maximize the effectiveness of both metformin and thyroid medications while minimizing potential complications. Levothyroxine, the most commonly prescribed thyroid hormone replacement, should be taken on an empty stomach, typically 30–60 minutes before breakfast or at bedtime (at least 3 hours after the last meal). This timing ensures optimal absorption, as food, particularly high-fiber meals, calcium, and iron supplements, can significantly reduce levothyroxine bioavailability. Calcium and iron supplements should be separated from levothyroxine by at least 4 hours.
Metformin is generally taken with meals to reduce gastrointestinal side effects, which are among the most common adverse reactions. Standard immediate-release metformin is typically dosed twice daily with breakfast and dinner, while extended-release formulations may be taken once daily with the evening meal. This creates a natural separation from morning levothyroxine dosing, which is advantageous for medication adherence and absorption.
Recommended timing approach:
Take levothyroxine first thing in the morning on an empty stomach
Wait at least 30–60 minutes before eating breakfast
Take metformin with breakfast and dinner (or as prescribed)
Maintain consistent timing daily for both medications
Dosage considerations require individualization based on patient-specific factors. Metformin is typically initiated at 500 mg once or twice daily, with gradual titration based on glycemic response and tolerability. Maximum doses vary by formulation: immediate-release up to 2,550 mg daily, while extended-release formulations generally max at 2,000 mg daily. Metformin is contraindicated if eGFR is below 30 mL/min/1.73m², and initiation is not recommended if eGFR is 30-45 mL/min/1.73m². Levothyroxine dosing is weight-based, typically 1.6 mcg/kg daily for complete thyroid replacement, but must be adjusted based on TSH monitoring.
Patients should not adjust doses of either medication without consulting their healthcare provider. If metformin is newly initiated in a patient stable on levothyroxine, thyroid function testing may be considered after 6–12 weeks to assess whether levothyroxine dose adjustment is needed.
Regular monitoring of thyroid function is essential for patients taking both metformin and thyroid medication to ensure therapeutic goals are met and to detect any necessary dose adjustments. The American Thyroid Association recommends checking TSH levels 6–8 weeks after initiating or changing levothyroxine doses, as this timeframe allows for steady-state hormone levels to be achieved.
For patients stable on levothyroxine who begin metformin therapy, clinicians may consider an additional TSH measurement 6–12 weeks after metformin initiation. This allows identification of any metformin-associated TSH changes that might warrant levothyroxine dose modification. Subsequently, annual TSH monitoring is generally sufficient for stable patients, though more frequent testing may be indicated based on symptoms or clinical circumstances.
Key monitoring parameters include:
TSH (primary marker for thyroid function assessment)
Free T4 (when TSH results are abnormal or symptoms persist)
Hemoglobin A1c (for diabetes management, typically every 3–6 months)
Vitamin B12 levels (periodic measurement, especially with anemia or neuropathy symptoms)
Renal function (at least annually; every 3–6 months if eGFR <60 mL/min/1.73m²)
Patients should discontinue biotin supplements at least 48 hours before thyroid function tests, as biotin can interfere with many thyroid assays and produce misleading results.
Patients should be educated about symptoms that might indicate thyroid hormone imbalance. Hypothyroid symptoms include fatigue, weight gain, cold intolerance, constipation, and depression, while hyperthyroid symptoms include anxiety, palpitations, heat intolerance, weight loss, and tremor. Any new or worsening symptoms should prompt contact with a healthcare provider rather than waiting for scheduled monitoring.
Maintaining a medication diary or using smartphone applications can help patients track symptoms, medication adherence, and laboratory results. This information proves valuable during clinical visits and facilitates informed decision-making regarding medication management. Patients should bring all medication bottles to appointments to verify dosing accuracy and discuss any concerns about their treatment regimen.
Certain situations require prompt consultation with your healthcare provider when taking metformin and thyroid medication concurrently. Understanding these scenarios empowers patients to seek timely medical attention and prevents potential complications.
Seek medical advice if you experience:
New or worsening symptoms of thyroid dysfunction (fatigue, weight changes, temperature intolerance, mood changes, palpitations)
Persistent gastrointestinal symptoms from metformin (severe diarrhea, nausea, vomiting, abdominal pain)
Signs of lactic acidosis (rare but serious): unusual muscle pain, difficulty breathing, severe weakness, dizziness, or slow/irregular heartbeat
Symptoms of hypoglycemia if taking metformin with other diabetes medications (shakiness, sweating, confusion, rapid heartbeat)
Acute illness, dehydration, or severe infection (may require temporary metformin discontinuation)
Any new medications or supplements are prescribed, as these may interact with thyroid medication absorption
Additional important situations requiring consultation:
If you are scheduled for a procedure using iodinated contrast media, as metformin may need to be temporarily discontinued depending on your kidney function and other risk factors
If you become pregnant or are planning pregnancy, as both thyroid hormone and diabetes medication requirements typically change significantly during pregnancy
Scheduled consultations are equally important. Patients should have regular follow-up appointments every 3–6 months when both medications are being adjusted, and at least annually once stable. These visits should include review of symptoms, medication adherence, laboratory results, and any necessary dose adjustments.
Patients should also consult their provider before starting any new over-the-counter medications or dietary supplements, particularly calcium, iron, or fiber supplements, which can interfere with levothyroxine absorption. Similarly, changes in diet, exercise routines, or other health conditions (particularly kidney or liver problems) may necessitate medication adjustments.
Never discontinue either medication without medical guidance, even if you feel well. Both metformin and thyroid medications require consistent use to maintain therapeutic benefits. If side effects are problematic, discuss alternatives with your healthcare provider rather than stopping treatment independently. Establishing open communication with your healthcare team ensures optimal management of both diabetes and thyroid conditions while minimizing risks associated with concurrent medication use.
Take levothyroxine first thing in the morning on an empty stomach, wait at least 30–60 minutes before eating breakfast, then take metformin with your meal. This natural separation optimizes absorption of both medications and minimizes gastrointestinal side effects from metformin.
Metformin may modestly reduce TSH levels by 0.4–1.5 mIU/L in some patients, particularly those with hypothyroidism taking levothyroxine, though free T4 and T3 levels typically remain stable. Healthcare providers may check TSH levels 6–12 weeks after starting metformin to determine if levothyroxine dose adjustment is needed.
No, metformin does not cause thyroid disease or dysfunction. While it may modestly influence TSH levels in some patients, this appears to be a modulatory effect rather than pathological, and patients with thyroid conditions should not avoid metformin based on these findings.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.