LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



As semaglutide (Ozempic, Wegovy, Rybelsus) becomes increasingly prescribed for type 2 diabetes and weight management, many patients of reproductive age wonder: can semaglutide cause infertility? Currently, no established scientific evidence demonstrates that semaglutide directly causes infertility in men or women. This GLP-1 receptor agonist works by mimicking natural hormones that regulate blood sugar and appetite, and the FDA does not list infertility as a known adverse effect. However, the medication's labeling includes specific pregnancy guidance, and significant weight changes can influence reproductive function through indirect pathways. Understanding the distinction between direct medication effects and metabolic consequences of weight loss is essential for informed treatment decisions during reproductive years.
Quick Answer: No established scientific evidence shows that semaglutide directly causes infertility in men or women.
Semaglutide is a glucagon-like peptide-1 (GLP-1) receptor agonist approved by the FDA for type 2 diabetes management (under the brand names Ozempic and Rybelsus) and chronic weight management (under the brand name Wegovy). As its use has expanded dramatically, particularly among individuals of reproductive age seeking weight loss, questions have emerged about potential effects on fertility.
Currently, there is no established scientific evidence that semaglutide directly causes infertility in men or women. The medication works primarily by mimicking the naturally occurring GLP-1 hormone, which enhances insulin secretion, suppresses glucagon release, slows gastric emptying, and reduces appetite through central nervous system pathways. While GLP-1 receptors are expressed in hypothalamic and reproductive pathways, human data do not demonstrate direct infertility effects.
However, the concern is not entirely unfounded. Significant weight changes—whether loss or gain—can affect reproductive function through various pathways. Additionally, the FDA labeling for semaglutide includes specific guidance regarding pregnancy, which has contributed to patient concerns about broader reproductive health implications. Understanding the distinction between direct medication effects and indirect consequences of weight loss is essential for patients and clinicians navigating treatment decisions during reproductive years.
This article examines the current evidence regarding semaglutide and fertility, explores how weight loss medications may influence reproductive function, reviews FDA guidance, and provides practical considerations for patient-provider discussions about reproductive health while using this medication.
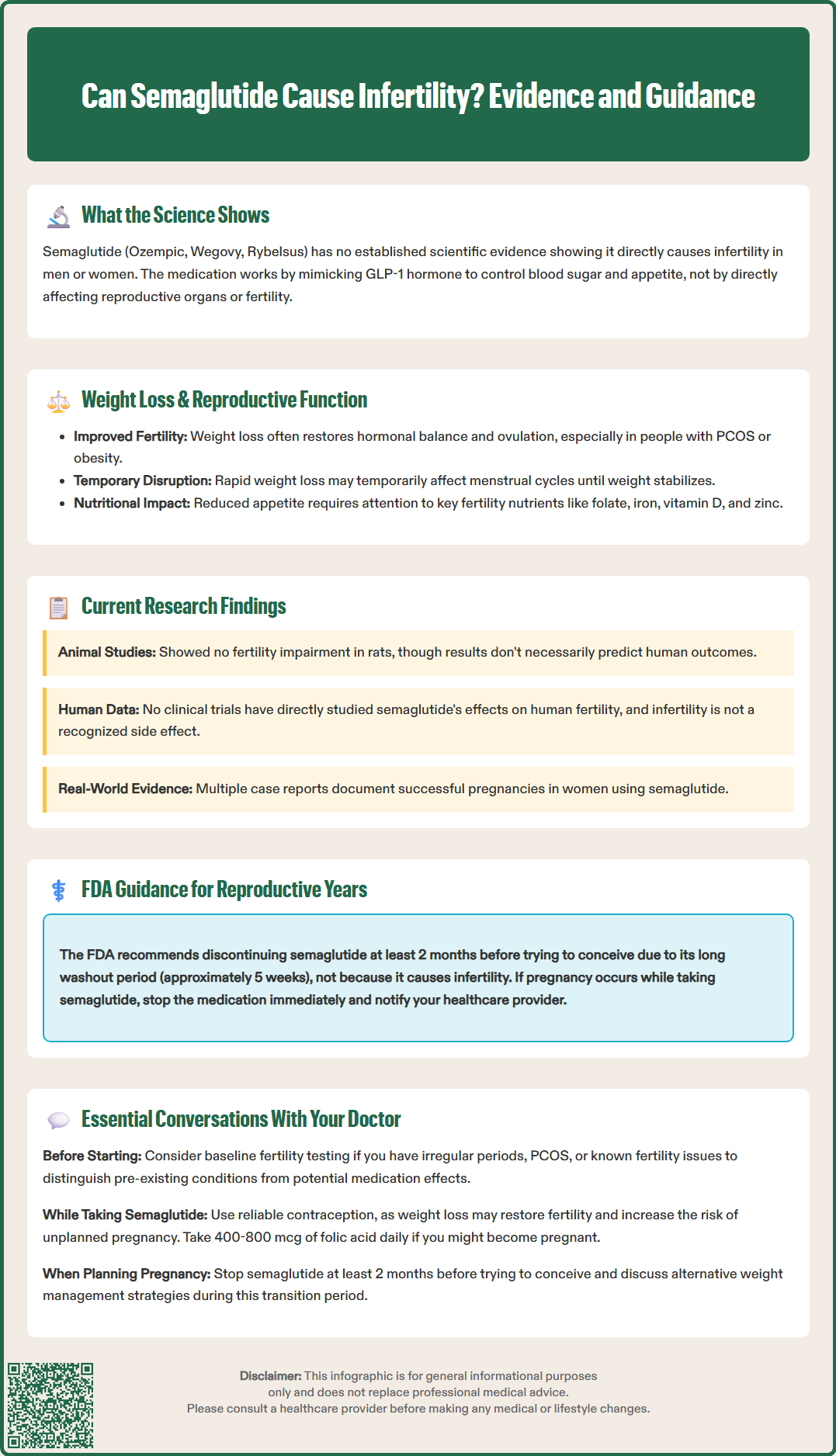
The existing research on semaglutide's direct effects on human fertility remains limited. Animal reproduction studies, required for FDA approval, have shown some findings that warrant consideration. In rat and rabbit studies, semaglutide was associated with embryo-fetal effects at exposures at, below, or above human therapeutic doses. Importantly, animal reproductive toxicity does not necessarily predict human outcomes, and the mechanisms observed in these studies may not translate directly to human physiology. Notably, animal studies did not show adverse effects on fertility parameters in rats.
No dedicated clinical trials have specifically evaluated semaglutide's impact on male or female fertility parameters in humans. The pivotal trials for both diabetes and weight management (SUSTAIN and STEP programs) excluded pregnant women and required contraception during participation, limiting our understanding of fertility effects. Post-marketing surveillance data have not identified infertility as a recognized adverse effect, though such passive reporting systems have inherent limitations in detecting subtle reproductive impacts.
Some observational evidence suggests that weight loss achieved through any method—including GLP-1 receptor agonists—may actually improve fertility in individuals with obesity-related reproductive dysfunction. Conditions such as polycystic ovary syndrome (PCOS) and obesity-associated anovulation often improve with weight reduction. Several case reports have documented pregnancies in women using semaglutide for weight loss, suggesting that improved metabolic health may restore ovulatory function rather than impair it.
The American Society for Reproductive Medicine has not issued specific guidance on semaglutide and fertility, reflecting the current evidence gap. The American Diabetes Association and American College of Obstetricians and Gynecologists provide broader guidance on preconception care that applies to GLP-1 receptor agonist use. Ongoing research, including real-world studies examining pregnancy outcomes in women exposed to semaglutide, may provide more definitive answers in coming years.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Weight loss medications, including semaglutide, can influence reproductive function through multiple indirect pathways, most of which relate to the metabolic changes accompanying weight reduction rather than direct drug effects on reproductive organs. Understanding these mechanisms helps contextualize fertility concerns.
Metabolic and hormonal improvements associated with weight loss often enhance fertility, particularly in individuals with obesity. Excess adipose tissue produces estrogen through aromatization of androgens, disrupting the hypothalamic-pituitary-gonadal axis. Weight loss can restore normal hormonal balance, potentially improving ovulation in women and sperm parameters in men. In women with PCOS—a leading cause of infertility—weight loss of just 5-10% can restore regular menstrual cycles and ovulation. This represents a fertility-enhancing rather than fertility-impairing effect.
However, rapid or excessive weight loss can temporarily disrupt reproductive function. Severe caloric restriction and significant body composition changes may trigger hypothalamic amenorrhea, where the brain suppresses reproductive hormone production in response to perceived energy deficit. This is typically reversible with weight stabilization and adequate nutrition. The rate of weight loss with semaglutide varies by dose, duration, and individual factors, and may be more rapid in the early weeks of treatment.
Gastrointestinal effects of semaglutide, including nausea and reduced appetite, may affect nutritional status if not properly managed. Adequate nutrition is essential for reproductive health, and deficiencies in key nutrients (iron, folate, vitamin D, zinc) can impact fertility. Patients should work with healthcare providers to ensure nutritional adequacy during treatment, including folic acid supplementation (400-800 mcg daily) for those who might become pregnant.
Regarding oral contraceptive efficacy, pharmacokinetic studies have not shown clinically meaningful effects of subcutaneous semaglutide on ethinyl estradiol/levonorgestrel exposure. While semaglutide delays gastric emptying, backup contraception is not generally required by the FDA label. However, if severe vomiting or diarrhea occurs, temporary additional contraceptive methods may be advisable, as with any medication that might cause significant gastrointestinal disturbance.
The FDA prescribing information for semaglutide provides specific guidance regarding use during reproductive years, primarily focused on pregnancy rather than fertility per se. Understanding this guidance is essential for patients of childbearing potential and their healthcare providers.
Semaglutide is classified as FDA Pregnancy Category: Not Assigned under the current labeling system (the previous letter category system was phased out). The prescribing information states that available data on semaglutide use in pregnant women are insufficient to determine drug-associated risks for major birth defects, miscarriage, or adverse maternal or fetal outcomes. Based on animal reproduction studies showing fetal harm at clinically relevant exposures, the FDA recommends that semaglutide should be discontinued at least 2 months before a planned pregnancy due to its long washout period (approximately 5 weeks after the last dose).
Weight loss medications, including semaglutide, are not recommended during pregnancy. If pregnancy occurs while taking semaglutide, the medication should be discontinued immediately, and the healthcare provider should be notified. For Wegovy specifically, patients can report pregnancy exposure to the manufacturer's pregnancy registry, which collects information about outcomes of pregnancies exposed to the medication.
This 2-month discontinuation recommendation reflects semaglutide's pharmacokinetics rather than evidence of direct fertility impairment. The medication has a half-life of approximately one week, and the FDA guidance ensures adequate clearance before conception to minimize any potential fetal exposure during early pregnancy, when organogenesis occurs.
For breastfeeding, the FDA notes that there are no data on semaglutide presence in human milk, effects on the breastfed infant, or effects on milk production. The developmental and health benefits of breastfeeding should be considered alongside the mother's clinical need for semaglutide and any potential adverse effects on the infant.
Importantly, the FDA labeling does not list infertility as a known adverse effect of semaglutide. The most common adverse reactions reported in clinical trials include gastrointestinal symptoms (nausea, vomiting, diarrhea, constipation), which occurred in a substantial proportion of patients but are generally transient. Healthcare providers should counsel patients that while pregnancy planning requires medication discontinuation, there is no evidence that semaglutide causes permanent reproductive harm or infertility.
Patients considering or currently using semaglutide who have concerns about fertility should engage in comprehensive discussions with their healthcare providers. Several key topics warrant attention to ensure informed decision-making and appropriate reproductive planning.
Pregnancy planning timeline is essential. Patients who are actively trying to conceive or planning pregnancy within the next few months should discuss whether initiating semaglutide is appropriate, given the FDA recommendation to discontinue the medication at least 2 months before planned conception. For those already using semaglutide who wish to become pregnant, establishing a clear timeline for discontinuation is important. Alternative weight management strategies during this transition period should be explored.
Contraception strategy requires careful consideration. Given that weight loss may restore fertility in some individuals with obesity-related reproductive dysfunction, unplanned pregnancy becomes a possibility. Patients should discuss reliable contraception methods, particularly if they are not planning pregnancy in the near term. Patients should be advised to take a pregnancy test if a menstrual period is missed and to discontinue semaglutide immediately if pregnancy occurs.
Baseline fertility assessment may be appropriate for some patients. Individuals with known or suspected fertility issues should consider evaluation before starting semaglutide, establishing baseline reproductive function. This is particularly relevant for women with irregular menstrual cycles, PCOS, or other reproductive conditions, and for men with known semen abnormalities. Documentation of baseline status helps distinguish pre-existing conditions from any potential medication effects.
Patients should be aware of infertility referral thresholds: generally after 12 months of attempting pregnancy for those under 35 years, or after 6 months for those 35 and older. Earlier evaluation is warranted with known risk factors such as irregular menses, amenorrhea lasting more than 3 months, severe male factor, endometriosis, or pelvic disease. Red flags requiring prompt evaluation include heavy or irregular bleeding, pelvic pain, galactorrhea, signs of androgen excess, or missed periods with negative pregnancy tests.
Monitoring during treatment should include attention to menstrual cycle changes, which may indicate either improved or disrupted reproductive function. Women should report new menstrual irregularities, though such changes may reflect positive metabolic improvements rather than adverse effects. Nutritional status monitoring is also important, ensuring adequate intake of fertility-relevant nutrients despite reduced appetite. Preconception folic acid supplementation (400-800 mcg daily) is recommended for women who might become pregnant.
Alternative treatment options should be discussed if fertility concerns are paramount. For weight management, lifestyle interventions or delaying pharmacotherapy until after desired pregnancies are completed may be considered. For diabetes management, insulin and sometimes metformin (in select cases) are preferred during pregnancy planning and pregnancy itself, per American Diabetes Association guidelines. Weight loss medications should be avoided during pregnancy.
Patients should feel empowered to ask direct questions: "Will this medication affect my ability to get pregnant?" "When should I stop this medication if I want to conceive?" "What contraception do you recommend while I'm taking this?" "Are there fertility tests I should have before starting?" Open communication ensures that treatment decisions align with individual reproductive goals and timelines, supporting both metabolic health and family planning objectives.
There is no established evidence that semaglutide directly impairs fertility in men or women. In fact, weight loss achieved with semaglutide may improve fertility in individuals with obesity-related reproductive dysfunction such as PCOS.
The FDA recommends discontinuing semaglutide at least 2 months before planned pregnancy due to its long washout period of approximately 5 weeks. This allows adequate medication clearance before conception to minimize potential fetal exposure during early pregnancy.
Yes, weight loss from semaglutide can improve fertility in individuals with obesity-related reproductive conditions. Weight reduction of 5-10% can restore regular menstrual cycles and ovulation in women with PCOS and improve hormonal balance in both men and women.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.