LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible




Creatine and tirzepatide interaction is a common concern for patients using tirzepatide (Mounjaro, Zepbound) for diabetes or weight management while considering creatine supplementation for muscle preservation. Tirzepatide is an FDA-approved dual GIP/GLP-1 receptor agonist that reduces appetite and improves glucose control, while creatine is a widely used supplement that enhances muscle performance and mass. No formal drug interaction exists between these substances, as they work through different mechanisms and metabolic pathways. However, considerations around kidney function monitoring, hydration status, and body composition tracking warrant careful clinical evaluation when using both concurrently.
Quick Answer: There is no documented drug interaction between creatine supplementation and tirzepatide, as they work through different mechanisms and metabolic pathways.
We offer compounded medications and Zepbound®. Compounded medications are prepared by licensed pharmacies and are not FDA-approved. References to Wegovy®, Ozempic®, Rybelsus®, Mounjaro®, or Saxenda®, or other GLP-1 brands, are informational only. Compounded and FDA-approved medications are not interchangeable.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Tirzepatide is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist approved by the FDA for type 2 diabetes management (marketed as Mounjaro) and chronic weight management (marketed as Zepbound).[1] This medication works by enhancing insulin secretion in response to meals, suppressing glucagon release, slowing gastric emptying, and reducing appetite.[1] In the SURMOUNT-1 clinical trial, higher doses in non-diabetic adults demonstrated significant weight loss, with participants losing approximately 15-20% of body weight over 72 weeks. Common adverse effects include gastrointestinal symptoms such as nausea, vomiting, diarrhea, and constipation, which typically diminish over time.[1] Important safety considerations include a boxed warning for thyroid C-cell tumors (medullary thyroid carcinoma/MEN2), and warnings for pancreatitis and gallbladder disease.[1]
Creatine is a naturally occurring compound synthesized in the liver, kidneys, and pancreas from amino acids (arginine, glycine, and methionine). It is also obtained through dietary sources, primarily meat and fish. Creatine phosphate serves as a rapid energy reserve in muscle tissue, particularly during high-intensity, short-duration activities. As a dietary supplement, creatine monohydrate is widely used to enhance athletic performance, increase muscle mass, and improve exercise capacity. The typical supplementation protocol involves a loading phase of 20 grams daily (divided into four doses) for 5-7 days, followed by a maintenance dose of 3-5 grams daily. Creatine supplementation causes intracellular water retention in muscle tissue, which accounts for initial weight gain of 2-4 pounds. Once in the body, creatine is primarily taken up by muscle tissue, with approximately 1-2% per day non-enzymatically converting to creatinine, which is then excreted by the kidneys.
| Interacting Substance | Effect | Risk Level | Advice |
|---|---|---|---|
| Creatine (general interaction with tirzepatide) | No documented drug-drug interaction; separate mechanisms and metabolic pathways | Low (healthy individuals) | No contraindication; disclose all supplements to prescribing physician |
| Creatine → Serum Creatinine / eGFR | May falsely elevate serum creatinine, underestimating true eGFR (creatinine-based) | Moderate (monitoring concern) | Use cystatin C-based eGFR or enzymatic assay if kidney function is in question (per KDIGO) |
| Tirzepatide GI effects → Creatine absorption | Nausea, vomiting, delayed gastric emptying may theoretically reduce creatine uptake | Low (theoretical) | Take creatine with meals; stabilize on tirzepatide 8–12 weeks before adding creatine |
| Tirzepatide-induced dehydration + Creatine | GI fluid losses combined with creatine's water demands may increase prerenal AKI risk | Moderate (volume-depleted patients) | Maintain adequate hydration; target pale yellow urine; seek care for persistent vomiting or low urine output |
| Creatine + Pre-existing Kidney Disease | Limited safety data in CKD; creatine metabolism adds creatinine load to impaired kidneys | High (eGFR <45 mL/min/1.73m²) | Nephrology referral for eGFR <30; co-management for eGFR <45; avoid without specialist guidance |
| Creatine water retention → Body weight scale | Initial 2–4 lb water weight gain may mask fat loss achieved by tirzepatide | Low (clinical interpretation) | Monitor waist circumference or body composition analysis rather than scale weight alone |
| Tirzepatide gastric emptying → Oral medications | Delayed gastric emptying may reduce absorption of narrow-therapeutic-index oral drugs | Moderate (drug-specific) | Review full medication list; oral contraceptive users need backup contraception for 4 weeks post-initiation or dose escalation |
There is no official contraindication or documented drug-drug interaction between creatine supplementation and tirzepatide in the FDA-approved prescribing information or major drug interaction databases (Lexicomp, Micromedex). These substances work through entirely different mechanisms and are metabolized via separate pathways. Tirzepatide is a peptide medication administered subcutaneously that undergoes proteolytic degradation, while creatine is a small organic compound absorbed in the small intestine and primarily taken up by muscle tissue before eventual conversion to creatinine.
The absence of a formal interaction does not mean combined use is without considerations. Many individuals taking tirzepatide for weight management may simultaneously use creatine to preserve or build lean muscle mass during caloric restriction—a reasonable approach given that GLP-1 receptor agonists can lead to loss of both fat and muscle tissue. The American Diabetes Association Standards of Care emphasizes the importance of resistance training and adequate protein intake during pharmacologic weight loss to maintain muscle mass, and creatine supplementation may support these goals.
However, no clinical trials have specifically evaluated the safety or efficacy of concurrent creatine and tirzepatide use. Healthcare providers should consider individual patient factors, including baseline kidney function, hydration status, and overall medication regimen. Patients should inform their prescribing physician about all supplements, including creatine, to ensure comprehensive monitoring and personalized recommendations. The decision to combine these substances should be made collaboratively, with attention to the specific clinical context and treatment objectives.
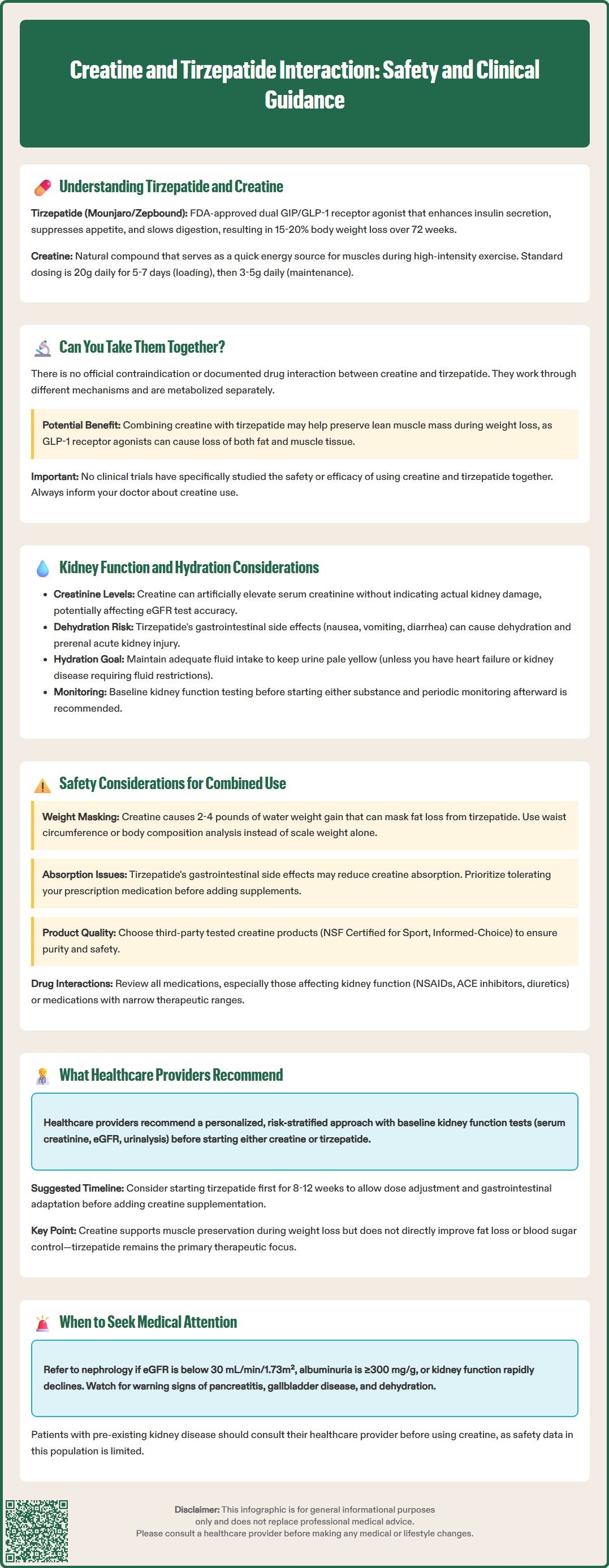
Kidney function monitoring deserves particular attention when considering combined use of creatine and tirzepatide. Creatine supplementation may modestly increase measured serum creatinine levels, which can confound creatinine-based estimated glomerular filtration rate (eGFR) calculations. This elevation reflects increased creatine metabolism rather than impaired kidney function. Clinicians should be aware that creatinine-based eGFR may underestimate true kidney function in creatine users. Alternative markers such as cystatin C-based eGFR or enzymatic creatinine assays may provide more accurate assessment when clinical concern exists, as recommended in KDIGO guidelines.
Tirzepatide itself has not been associated with direct nephrotoxicity. However, the medication's gastrointestinal effects—particularly nausea, vomiting, and diarrhea—can lead to dehydration and prerenal acute kidney injury if fluid intake is inadequate. The prescribing information includes warnings about acute kidney injury, particularly in patients experiencing volume depletion.[1] Additionally, tirzepatide can reduce the absorption of oral medications due to delayed gastric emptying, including oral contraceptives; patients using oral contraceptives should consider backup contraception for 4 weeks after tirzepatide initiation or dose escalation.
Hydration status becomes important with concurrent use. Creatine supplementation is associated with intracellular water retention in muscle tissue. Patients should maintain adequate fluid intake based on individual needs, with the goal of maintaining pale yellow urine color. Fluid recommendations should be individualized, particularly for patients with heart failure or kidney disease who may require fluid restrictions. Patients should contact their healthcare provider if they experience persistent or severe dehydration symptoms, orthostatic dizziness, inability to keep fluids down, or very low urine output. Baseline kidney function testing before initiating either substance, with periodic monitoring based on individual risk factors, represents prudent clinical practice, particularly in patients with diabetes or other kidney disease risk factors.
Several safety considerations merit attention when patients use creatine and tirzepatide concurrently. First, individuals with pre-existing kidney disease should discuss creatine supplementation with their healthcare provider. While research has not definitively shown that creatine worsens kidney function in healthy individuals, data in those with established kidney disease remain limited. According to FDA labeling, tirzepatide does not require dose adjustment for any degree of renal impairment, including end-stage renal disease.
Second, the gastrointestinal effects of tirzepatide may affect creatine absorption and tolerance. Nausea and delayed gastric emptying could theoretically reduce creatine uptake, though no studies have examined this interaction. Patients experiencing significant gastrointestinal symptoms should focus on tolerating their prescription medication before adding supplements. Taking creatine with meals may improve tolerance and absorption.
Third, weight and body composition monitoring becomes more complex with combined use. Creatine causes initial water weight gain of 2-4 pounds, which may mask fat loss achieved through tirzepatide. Patients should be counseled that scale weight may not accurately reflect body composition changes. Alternative metrics such as waist circumference, body composition analysis, or progress photographs provide better assessment of treatment efficacy.
Additional considerations include:
Medication interactions: Both substances should be reviewed in the context of the complete medication regimen, particularly other drugs affecting kidney function (NSAIDs, ACE inhibitors, diuretics) and medications with narrow therapeutic indices that may be affected by tirzepatide's effect on gastric emptying
Tirzepatide-specific risks: Patients should be counseled on the boxed warning for thyroid C-cell tumors, and signs/symptoms of pancreatitis and gallbladder disease
Hypoglycemia risk: When tirzepatide is used with insulin or sulfonylureas, dose reductions of these medications may be needed with glucose monitoring[1]
Quality of supplements: Creatine products should be third-party tested (NSF Certified for Sport, Informed-Choice) to ensure purity and absence of contaminants
Individual risk factors: Age over 65, diabetes duration, cardiovascular disease, and concurrent nephrotoxic medications increase risk
Monitoring parameters: Regular assessment of kidney function, hydration status, and electrolytes
Healthcare providers generally adopt a personalized, risk-stratified approach to patients considering concurrent creatine and tirzepatide use. The American College of Physicians and American Diabetes Association emphasize shared decision-making and individualized treatment plans for diabetes and weight management. When patients express interest in combining these substances, clinicians should conduct a thorough assessment including medical history, current medications, baseline kidney function, and treatment goals.
Recommended clinical approach includes:
Baseline evaluation: Consider obtaining serum creatinine, eGFR, and urinalysis before initiating either substance. Document baseline weight and body composition if possible.
Staged initiation: Consider starting tirzepatide first, allowing 8-12 weeks for dose titration and gastrointestinal adaptation before adding creatine supplementation.
Monitoring schedule: In high-risk patients, consider rechecking kidney function 4-6 weeks after starting creatine; otherwise, follow standard monitoring per diabetes and CKD care guidelines.
Hydration counseling: Provide individualized guidance on fluid intake based on comorbidities, with emphasis on maintaining pale yellow urine and adjusting intake during exercise or illness. Patients with heart failure or advanced kidney disease may require specific fluid restrictions.
Symptom education: Instruct patients on tirzepatide's boxed warning, signs of pancreatitis and gallbladder disease, and to report persistent dehydration, decreased urination, or unusual symptoms.
Most providers support creatine supplementation in appropriate candidates—particularly those engaged in resistance training to preserve muscle mass during weight loss. The International Society of Sports Nutrition position stand affirms creatine's safety profile in healthy individuals when used as directed. However, nephrology referral is appropriate for patients with eGFR <30 mL/min/1.73m², albuminuria ≥300 mg/g, rapid decline in kidney function, or complications. Consider co-management for eGFR <45 mL/min/1.73m².
Providers should also address realistic expectations: creatine supports muscle performance and may help maintain lean mass, but it does not directly enhance fat loss or improve glycemic control. The primary benefits of tirzepatide—improved glucose management and weight reduction—remain the therapeutic focus, with creatine serving as an adjunct to support body composition goals when clinically appropriate.
There is no official contraindication between creatine and tirzepatide, and no documented drug interaction exists in FDA labeling or major drug databases. However, patients should inform their healthcare provider about creatine use to ensure appropriate kidney function monitoring and hydration management.
Creatine supplementation may modestly increase serum creatinine levels, which reflects increased creatine metabolism rather than impaired kidney function. Patients with pre-existing kidney disease should discuss creatine use with their provider, and baseline kidney function testing with periodic monitoring is recommended.
Creatine causes intracellular water retention in muscle tissue, leading to initial weight gain of 2-4 pounds that may mask fat loss from tirzepatide on the scale. However, creatine can help preserve lean muscle mass during weight loss, which is beneficial for long-term metabolic health and body composition.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.