LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible



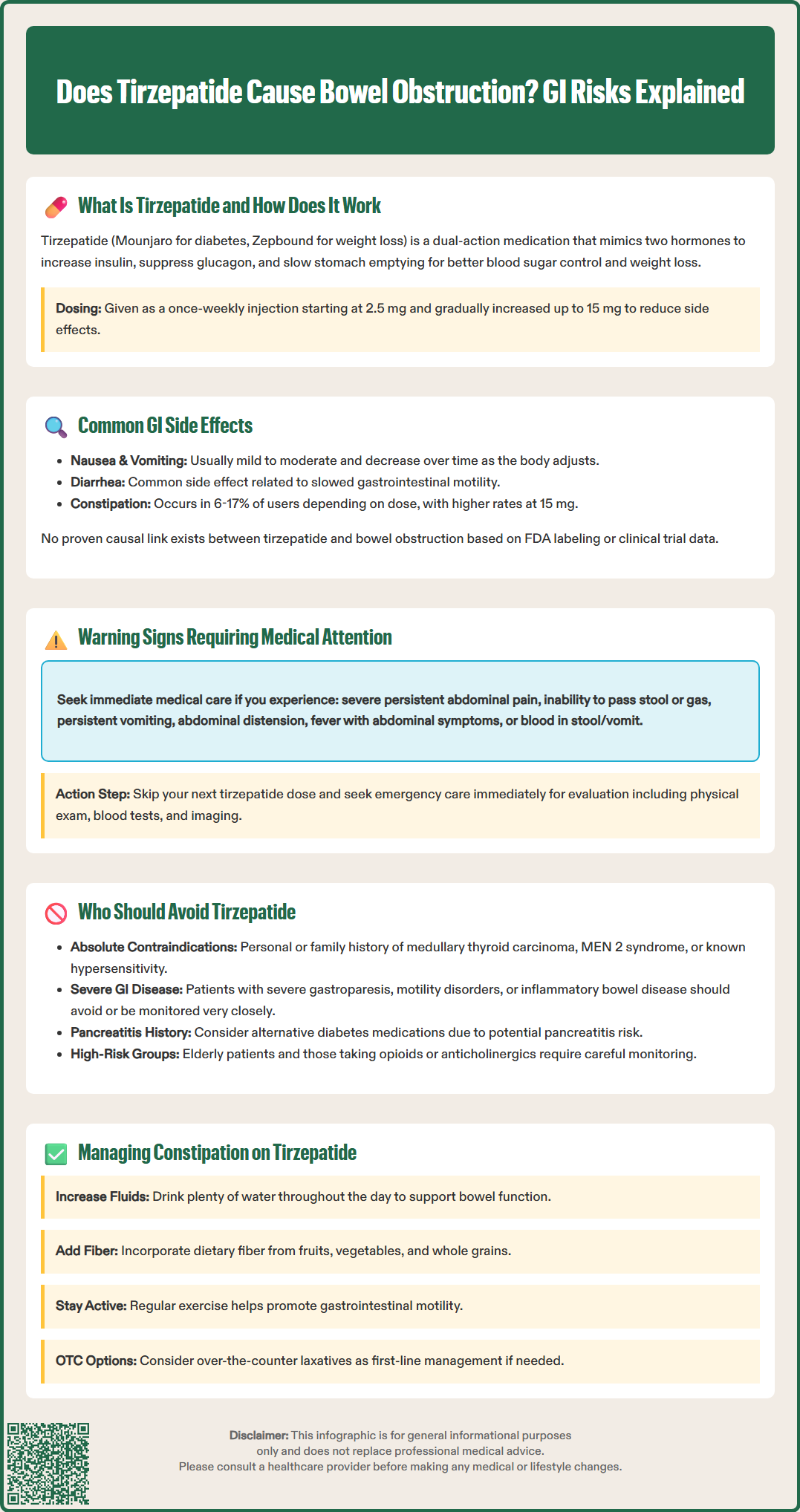
Does tirzepatide cause bowel obstruction? This question concerns many patients and clinicians considering this dual GIP/GLP-1 receptor agonist for type 2 diabetes or weight management. Tirzepatide (Mounjaro, Zepbound) slows gastric emptying and gastrointestinal motility, leading to common side effects like nausea and constipation. While bowel obstruction is not established as a recognized adverse effect in FDA labeling or clinical trials, understanding the gastrointestinal risks, warning signs, and patient populations who should avoid tirzepatide is essential for safe prescribing and monitoring.
Quick Answer: Bowel obstruction is not an established adverse effect of tirzepatide in FDA labeling or clinical trials, though the medication slows gastrointestinal motility and causes constipation in 6-17% of patients.
Tirzepatide is a novel glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist approved by the FDA for the treatment of type 2 diabetes mellitus under the brand name Mounjaro and for chronic weight management as Zepbound. As a dual incretin mimetic, tirzepatide enhances insulin secretion in a glucose-dependent manner, suppresses glucagon release, and slows gastric emptying—mechanisms that collectively improve glycemic control and promote weight loss.
The pharmacological action of tirzepatide on the gastrointestinal tract is central to both its therapeutic efficacy and its adverse effect profile. The delayed gastric emptying effect is primarily mediated through GLP-1 receptor activation and contributes to increased satiety and reduced caloric intake, which are beneficial for weight management. This effect may show some tachyphylaxis (diminishing response) with continued use. However, this same mechanism also underlies many of the gastrointestinal side effects reported by patients.
Tirzepatide is administered as a once-weekly subcutaneous injection, with doses ranging from 2.5 mg to 15 mg. The 2.5 mg dose is used only for initiation and is not intended for glycemic control. The medication is typically initiated at this lower dose and gradually titrated upward to minimize gastrointestinal adverse effects. Clinical trials have demonstrated significant reductions in hemoglobin A1c and body weight, making tirzepatide an important therapeutic option for patients with type 2 diabetes and obesity.
Importantly, according to FDA labeling, tirzepatide is not recommended in patients with severe gastrointestinal disease, including severe gastroparesis. Understanding its mechanism of action is essential for clinicians to anticipate potential gastrointestinal complications and counsel patients appropriately.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Gastrointestinal adverse effects are the most commonly reported side effects associated with tirzepatide therapy. In pivotal clinical trials, nausea, diarrhea, vomiting, constipation, abdominal pain, and dyspepsia were frequently observed, particularly during dose escalation. These effects are generally mild to moderate in severity and tend to diminish over time as patients develop tolerance to the medication. The incidence of gastrointestinal side effects is dose-dependent, with higher rates observed at the 10 mg and 15 mg doses compared to lower doses.
Constipation is a particularly relevant adverse effect when considering the question of bowel obstruction risk. In clinical trials, constipation was reported in approximately 12-17% of patients receiving tirzepatide for obesity (Zepbound) and 6-15% of patients with type 2 diabetes (Mounjaro), with higher rates at the 15 mg dose. Constipation can range from mild infrequent bowel movements to more severe cases requiring intervention. The slowed gastrointestinal motility induced by tirzepatide can contribute to stool retention and increased colonic transit time.
Currently, there is no established causal link between tirzepatide and bowel obstruction in the FDA-approved prescribing information or published clinical trial data. Bowel obstruction has not been identified as a recognized adverse effect in the large phase 3 trials that led to tirzepatide's approval. However, the FDA has added ileus to the labeling of another GLP-1 receptor agonist (semaglutide) in postmarketing surveillance, suggesting a potential class effect that warrants monitoring. The FDA labeling for tirzepatide does include warnings about severe gastrointestinal adverse reactions, as well as risks of dehydration, acute kidney injury, and acute gallbladder disease.
Patients experiencing persistent constipation should be counseled on conservative management strategies, including increased fluid intake, dietary fiber supplementation, physical activity, and over-the-counter laxatives when appropriate. If constipation becomes severe or is accompanied by other concerning symptoms, further evaluation is warranted to rule out complications.
While most gastrointestinal side effects of tirzepatide are self-limiting and manageable, certain warning signs should prompt immediate medical evaluation. Patients and clinicians must be able to distinguish between expected adverse effects and symptoms that may indicate serious complications such as bowel obstruction, ileus, or other acute abdominal pathology.
Red flag symptoms that require urgent assessment include:
Severe, persistent abdominal pain that is constant or progressively worsening, particularly if localized or associated with abdominal distension
Inability to pass stool or gas, especially if accompanied by cramping, bloating, or pain
Persistent nausea and vomiting that prevents oral intake or leads to dehydration
Abdominal distension with a visibly swollen or tense abdomen
Fever in conjunction with abdominal symptoms, which may suggest perforation or peritonitis
Blood in stool or vomit, which could indicate mucosal injury or ischemia
Bowel obstruction typically presents with colicky abdominal pain, distension, vomiting (which may become feculent in complete obstruction), and obstipation (inability to pass stool or flatus). Physical examination may reveal high-pitched bowel sounds early in the course or absent bowel sounds in complete obstruction. Computed tomography (CT) of the abdomen and pelvis is usually the preferred diagnostic imaging modality for suspected bowel obstruction, offering better sensitivity and specificity than plain radiographs.
Patients taking tirzepatide who develop these symptoms should hold their next dose and seek immediate medical attention. Emergency department evaluation should include a thorough history, physical examination, laboratory studies (complete blood count, comprehensive metabolic panel), and appropriate imaging. Early recognition and intervention are critical to prevent complications such as bowel ischemia, perforation, or sepsis. Clinicians prescribing tirzepatide should provide clear safety netting advice and ensure patients understand when to seek urgent care.
Certain patient populations may be at increased risk for gastrointestinal complications with tirzepatide and should either avoid the medication or be monitored closely if treatment is deemed necessary. The FDA prescribing information provides specific contraindications and warnings that guide clinical decision-making.
Absolute contraindications include:
Personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN 2)
Known hypersensitivity to tirzepatide or any excipients
According to FDA labeling, tirzepatide is not recommended in patients with severe gastrointestinal disease, including severe gastroparesis. Additionally, the following conditions may warrant careful consideration based on clinical judgment, though evidence specifically linking these conditions to increased risk with tirzepatide is limited:
History of significant gastrointestinal motility disorders that could be exacerbated by further slowing of gastric emptying
Inflammatory bowel disease with active inflammation or history of stricturing complications
Recent abdominal surgery, particularly procedures involving the gastrointestinal tract
Severe chronic constipation that is difficult to manage
Regarding pancreatitis, the FDA label advises clinicians to consider alternative antidiabetic therapy in patients with a history of pancreatitis, as GLP-1 receptor agonists have been associated with acute pancreatitis in some cases.
Additionally, elderly patients and those with multiple comorbidities may be more vulnerable to dehydration and electrolyte disturbances from gastrointestinal side effects. Patients taking medications that slow gastrointestinal motility (such as opioids or anticholinergics) may experience additive effects and should be counseled accordingly.
Importantly, tirzepatide may reduce the absorption of oral medications due to delayed gastric emptying. The FDA label specifically notes reduced exposure to oral contraceptives during tirzepatide initiation and dose escalation; patients should be advised to use a non-oral contraceptive method or add a barrier method for 4 weeks after initiation and each dose increase.
Before initiating tirzepatide, clinicians should obtain a thorough gastrointestinal history and discuss the potential for adverse effects. Shared decision-making is essential, weighing the metabolic benefits against individual risk factors. For patients at higher risk, alternative therapies should be considered, and if tirzepatide is prescribed, close monitoring with a lower starting dose and slower titration schedule may be appropriate.
Tirzepatide commonly causes gastrointestinal side effects like nausea and constipation, but bowel obstruction is not an established adverse effect in clinical trials or FDA labeling. Patients with severe gastrointestinal disease should avoid tirzepatide.
Warning signs include severe persistent abdominal pain, inability to pass stool or gas, persistent vomiting, abdominal distension, and fever with abdominal symptoms. These symptoms require immediate medical evaluation and holding the next dose.
Tirzepatide is not recommended for patients with severe gastrointestinal disease including severe gastroparesis. Clinicians should carefully consider use in patients with significant motility disorders, inflammatory bowel disease with strictures, or severe chronic constipation.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.