LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
- Your personalised programme is built around medical care, not willpower.
- No generic diets. No guesswork.
- Just science-backed results and expert support.
Find out if you’re eligible




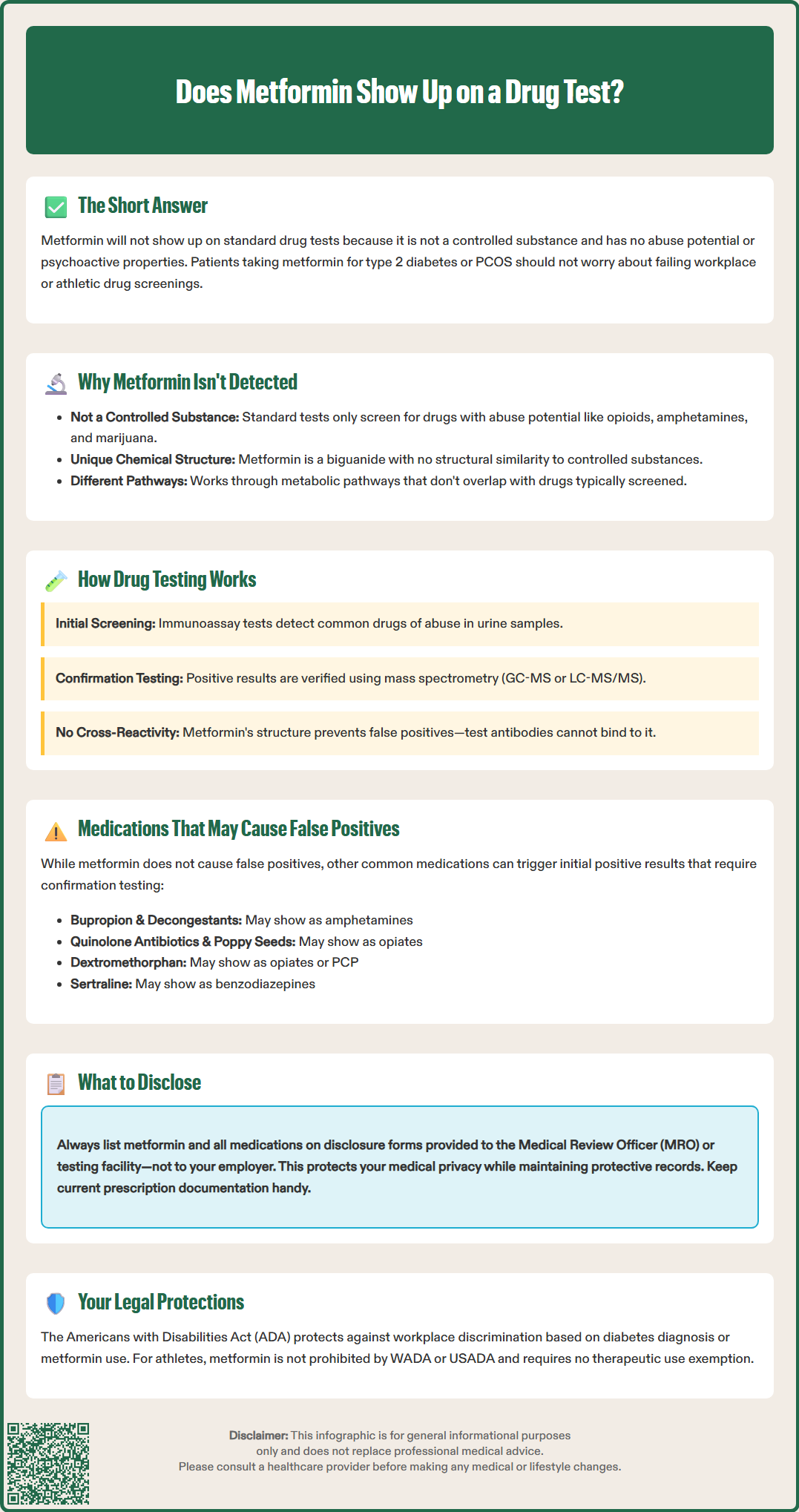
Does metformin show up on a drug test? This common question concerns many patients prescribed this first-line diabetes medication. Metformin, a biguanide antidiabetic agent used to manage type 2 diabetes and sometimes polycystic ovary syndrome (PCOS), is not detected by standard drug screening panels. Unlike controlled substances with abuse potential, metformin has no psychoactive properties and is not included in routine workplace, athletic, or law enforcement drug tests. Understanding how drug testing works and what substances are actually screened can help patients taking metformin navigate employment and athletic requirements with confidence.
Quick Answer: Metformin does not show up on standard drug tests because it is not a controlled substance and has no abuse potential.
Metformin is not expected to show up on standard drug tests used by employers, athletic organizations, or law enforcement agencies. This medication, prescribed for type 2 diabetes and sometimes off-label for polycystic ovary syndrome (PCOS) in the US, is not a controlled substance and is not included in routine drug screening panels.
Standard drug tests are designed to detect substances with abuse potential, including opioids, amphetamines, benzodiazepines, marijuana, and cocaine. Metformin, a biguanide antidiabetic medication, has no psychoactive properties and carries virtually no risk of dependence or abuse. The FDA-approved drug label for metformin does not classify it as a controlled substance under the Controlled Substances Act.
Metformin works by decreasing hepatic glucose production, reducing intestinal glucose absorption, and improving insulin sensitivity in peripheral tissues. Its mechanisms involve multiple pathways, including effects on AMP-activated protein kinase (AMPK), mitochondrial complex I, and mitochondrial glycerophosphate dehydrogenase. These pathways have no overlap with the pharmacological targets of substances typically screened in drug tests. The medication is eliminated primarily unchanged through the kidneys, with a plasma elimination half-life of approximately 6.2 hours in patients with normal renal function.
Patients taking metformin for legitimate medical purposes should not be concerned about positive drug test results related to this medication. While specialized tests could detect metformin if specifically designed to do so, such targeted testing is not part of standard drug-of-abuse panels. Understanding what drug tests actually detect and how certain medications might interfere with testing can help patients navigate workplace or athletic drug screening requirements with confidence.
LOSE WEIGHT WITH MEDICAL SUPPORT — BUILT FOR MEN
Find out if you’re eligible

Drug testing typically employs immunoassay screening methods as the initial step, followed by confirmatory testing using gas chromatography-mass spectrometry (GC-MS) or liquid chromatography-tandem mass spectrometry (LC-MS/MS) for positive results. Immunoassays use antibodies designed to bind to specific drug molecules or their metabolites in urine, blood, saliva, or hair samples.
The standard federal drug testing panel in the US, as defined by the Department of Health and Human Services (HHS) and the Substance Abuse and Mental Health Services Administration (SAMHSA), includes:
Marijuana (THC metabolites) – typically detectable in urine for 3–30 days depending on usage patterns
Cocaine metabolites – usually detectable in urine for 2–4 days after use
Opiates (morphine, codeine) – generally detectable in urine for 2–3 days
Amphetamines and methamphetamine – typically detectable in urine for 2–4 days
Phencyclidine (PCP) – can be detected in urine for up to 8 days
Semi-synthetic opioids (oxycodone, oxymorphone, hydrocodone, hydromorphone) – added to federal panels in 2017
Detection windows vary considerably based on dose, frequency of use, individual metabolism, and the specific specimen type being tested. The times listed above refer to urine testing, the most common matrix used.
Expanded panels may include additional substances such as benzodiazepines, barbiturates, methadone, fentanyl, buprenorphine, and synthetic cannabinoids. Federal workplace drug testing programs follow standardized protocols with specific cutoff concentrations established by SAMHSA to minimize false positives.
Immunossay tests are designed with antibodies that recognize specific epitopes (binding sites) on target drug molecules. Metformin's chemical structure—a biguanide with the formula C₄H₁₁N₅—bears no structural similarity to controlled substances. The antibodies used in standard drug panels will not bind to metformin, making cross-reactivity extremely unlikely.
Confirmatory testing using mass spectrometry provides definitive identification by measuring the exact molecular weight and fragmentation pattern of detected substances. This highly specific method would clearly distinguish metformin from any controlled substance, though metformin would not trigger the initial immunoassay screen in the first place.
While metformin does not cause false positive drug tests, several legitimate prescription and over-the-counter medications can trigger initial positive results on immunoassay screening. The likelihood of false positives varies significantly by immunoassay manufacturer, testing platform, and cutoff thresholds used.
Medications that may cause false positives include:
Amphetamines panel: Bupropion (Wellbutrin), pseudoephedrine, phenylephrine, labetalol, trazodone, and some decongestants may trigger false positives. Cross-reactivity varies by assay type and manufacturer.
Opiates panel: Quinolone antibiotics (ciprofloxacin, levofloxacin) and poppy seed consumption can cause false positive results, though modern federal testing uses higher cutoffs that reduce poppy seed interference. Dextromethorphan, found in many cough suppressants, may occasionally cross-react with certain assays.
Benzodiazepines panel: Sertraline (Zoloft) and oxaprozin (a nonsteroidal anti-inflammatory drug) have been reported to cause false positives in some immunoassay systems.
Marijuana panel: Some older immunoassays showed cross-reactivity with certain NSAIDs and proton pump inhibitors, though this is increasingly rare with modern testing platforms. Efavirenz (an HIV medication) may still cause false positives on some THC assays.
Phencyclidine (PCP) panel: Dextromethorphan, diphenhydramine, tramadol, and venlafaxine have been associated with false positive PCP results in certain immunoassay systems.
The HHS Mandatory Guidelines for Federal Workplace Drug Testing Programs require that all presumptive positive immunoassay results be confirmed with more specific testing methods (GC-MS or LC-MS/MS) before any adverse action is taken. This confirmatory testing will definitively identify the actual substance present, clearing patients taking legitimate medications.
Patients should be aware that while initial screening may occasionally produce false positives with certain medications, metformin is not among the medications known to cause such interference. Its chemical structure and pharmacological profile make cross-reactivity with standard drug test antibodies highly unlikely.
Patients taking metformin generally do not need to disclose this medication specifically for drug testing purposes, as it will not affect test results. However, providing complete medication information to the Medical Review Officer (MRO) or testing facility is considered best practice and can prevent unnecessary complications.
Recommended disclosure approach:
When undergoing pre-employment, random, or for-cause drug testing, patients should complete any medication disclosure forms accurately and thoroughly. List all prescription medications, including metformin, along with the prescribing physician's contact information. This information should be provided to the MRO or collection site personnel—not directly to employer HR departments—to maintain medical privacy. This documentation serves as a protective record should any questions arise, though metformin itself poses no testing concerns.
If a drug test produces an unexpected positive result, the MRO—a licensed physician responsible for reviewing test results—will contact the individual to discuss potential explanations. At this point, providing a complete list of all medications, including metformin and any other prescriptions or over-the-counter drugs, helps the MRO determine whether a legitimate medication could explain the finding.
Patient safety considerations:
Patients should maintain current documentation of their metformin prescription, including:
Prescription bottle with pharmacy label showing medication name, dosage, and prescriber
Letter from prescribing physician if requested by testing facility
Updated medication list for personal records
For patients taking metformin alongside other medications that might cause false positives (such as those listed in the previous section), proactive disclosure to the MRO becomes more important. Inform the testing facility before the test about all medications that could potentially interfere with results.
The Americans with Disabilities Act (ADA) provides protections for individuals with diabetes and other medical conditions. Employers cannot discriminate based on diabetes diagnosis or the use of medications like metformin to manage the condition. If concerns arise about disclosure or workplace discrimination related to diabetes medication use, patients should consult with their healthcare provider and may wish to seek guidance from an employment attorney or the Equal Employment Opportunity Commission (EEOC).
In athletic or competitive settings, metformin is not prohibited by the World Anti-Doping Agency (WADA) or the United States Anti-Doping Agency (USADA). Athletes taking metformin do not require therapeutic use exemptions, though maintaining documentation of legitimate medical use remains advisable.
No, metformin does not cause false positive drug test results. Its chemical structure as a biguanide bears no similarity to controlled substances, and standard immunoassay antibodies will not bind to metformin molecules.
While metformin will not affect drug test results, providing complete medication information to the Medical Review Officer is considered best practice. This maintains a protective record while preserving medical privacy from direct employer access.
No, metformin is not prohibited by the World Anti-Doping Agency (WADA) or United States Anti-Doping Agency (USADA). Athletes taking metformin do not require therapeutic use exemptions, though maintaining documentation of legitimate medical use is advisable.
All medical content on this blog is created using reputable, evidence-based sources and is regularly reviewed for accuracy and relevance. While we strive to keep our content current with the latest research and clinical guidelines, it is intended for general informational purposes only.
This content is not a substitute for professional medical advice, diagnosis, or treatment. Always consult a licensed healthcare provider with any medical questions or concerns. Use of this information is at your own risk, and we are not liable for any outcomes resulting from its use.